[vc_row][vc_column][vc_column_text]
“How Do You PQI?”
This is phrase that COA came up with a few years ago to introduce our newest toolkit. As an accreditation insider, we think it’s a clever phrase in that it conveys that:
- PQI is a necessity
- PQI is something that you do and that has motion, and
- PQI is customizable.
(We also like that it rolls off the tongue easily, unlike the word “accreditation.”)
Unfortunately, not everyone is an accreditation insider. We love our acronyms at COA, and use them everywhere–in our standards, in our process, in our technology (shout out to the VIP portal!). But acronyms and jargon can be confusing to anyone not in the know, and create barriers to understanding. “PQI” is no different.
So what is PQI, you ask?
Good question–and a common question we’re asked when staffing COA’s exhibit booth at a conference. The conversation usually goes something like this:
Inquiring person: What is PQI?
Us: It’s the foundation of the accreditation process.
Inquiring Person: Yes, but what does it mean?
Us: “Performance and Quality Improvement.” It’s our name for Quality Improvement or Quality Assurance.
Inquiring person: Thanks. What’s “Quality Improvement”?
Us: On a basic level, we like to say that a PQI system is collecting data about your work, analyzing it, making course-corrections based on the data, and then tracking to see if those changes are working.
Then we usually see a glimmer of understanding in their eyes. We give the inquiring person our PQI Toolkit postcard, and hope that it makes its way to the Quality Assurance/Data Nerd at their agency.
Based on our conversations with stakeholders, in-process organizations, and peers, we at COA know that PQI is can be a conceptual, difficult-to-grasp concept. We also know that agencies need a lot of help developing their PQI systems. This is why we talk about PQI a lot, and why we create trainings and tools to help.
One long-awaited tool is a high-level introduction to PQI for anyone new to the concept. Now when we’re manning the exhibit table and get asked “What is PQI?”, we are thrilled to be able to reply:
“Check out our PQI whiteboard video!”
Transcript
The most effective social service organizations are those that have been accredited to meet the highest standards of quality.
For more than 40 years, the nonprofit Council on Accreditation has partnered with health and human service organizations globally to improve outcomes by developing, applying, and promoting accreditation standards.
COA’s Performance and Quality Improvement standards, or PQI, require organizations to generate and review organization-wide data to establish performance targets that improve services and outcomes for all stakeholders. It’s a comprehensive process that includes working with the entire organization instead of assigning the responsibility for quality improvement to just a few individuals.
Information generated by the PQI system is used to:
- Monitor progress toward achievement of strategic goals and long-term direction,
- Manage programs and operations efficiently and effectively,
- Meet funder requirements to promote the organization and its services throughout the community, and
- Support direct service staff to meet program goals and have a positive impact on people served.
The organization reviews findings and feedback while taking action to:
- Eliminate or reduce identified challenges,
- Replicate good practices,
- Recognize and motivate staff, and
- Improve services for the communities they serve and assist with fulfilling their mission.
And hopefully now you think the phrase “How Do You PQI?” is clever, too.
Want to dig deeper into PQI? Check out our comprehensive PQI Toolkit.
[/vc_column_text][/vc_column][/vc_row]
Your organization has decided to embark on the journey of pursuing accreditation! This commitment can invoke many sentiments—happiness, anticipation, fear, anxiety, and maybe even a splash of frustration. These are all normal feelings. The accreditation process is a major project with a myriad of components. One way to be successful in your accreditation work is to use a project management approach, as it is critical to divide the required work into smaller, manageable steps. Here is a handy, step-by-step guide you can use to conceptualize the tasks that are on the horizon.
Work styles & organizational culture
COA has an organization-wide accreditation model. This means that not only are programs being reviewed, but also the administrative divisions as well. Getting many colleagues involved in the accreditation process will help the organization manage the workload and focus on developing, updating, or sustaining practices that are ultimately in the best interest of the consumers served.
People have different personalities, which includes varied preferences and approaches to their work responsibilities. There are those who are process-oriented people that do a really great job poking holes in plans and asking questions that may not have been considered. Then there are staff who can reflect and acknowledge the progress that has been made within the organization through that point in time. Knowing some of these characteristics and preferences will be helpful in thinking about who should handle different aspects of the work.
How and why the organization is choosing to pursue accreditation is essential to framing the work that lies ahead. Even if the organization is mandated to achieve accreditation, what the organization hopes to accomplish through this process is valuable for all to hear. Ask yourself: What is the message we will convey to our board, advisory group, staff, consumers, and other relevant stakeholders about what accreditation means for the organization and its future? People want something they can believe in, something that resonates with them, so taking time to reflect and think about the “why” behind this journey is an opportunity to capitalize on building momentum.
Accreditation workload – forming the structure
COA accreditation includes all aspects of the organization’s administration and service delivery operations. There are three types of standards: administration and management, service delivery administration, and service. Most organizations will have at least ten standard sections to review based on the three categories. It is essential to have multiple staff managing different standard sections, because no one staff member will have all the answers (and that is a good thing)!
A question we often hear from organizations is “How will we manage the accreditation work?” You must consider whether your organizational structure serves as a sufficient framework to review the standards. This means that those individuals responsible for particular divisions would delegate tasks to staff within their department. For example, the director of human resources would review the human resources management standard section and assign tasks as needed to his/her staff. Similarly, program directors would follow the same process to review service standard areas.
Another option for managing the work includes the creation of functional work groups, which includes assembling teams with individuals from different departments and/or programs to review one or more standard sections. For example, an administrative work group can be formed to review multiple standard areas including risk management, administrative service environment, ethical practice, etc. This type of work group would include an interdisciplinary team of quality improvement, program, information technology, and other staff as needed.
Decision-making authority and flow of communication
Once a decision is made on whether to use the structural work groups, functional work groups, or a hybrid of the two, the organization must consider the decision-making authority. As teams begin to work on reviewing the standards against current practices, you may find that policies, procedures, and protocols may need to be developed or modified. The organization must be clear on who has the authority to implement new procedures and practices.
Typically, if hierarchical work groups are used, the head of the department or program would be responsible for managing the approval process. Larger organizations may have a chief operations officer or director, and that person may be responsible for final approval. In smaller organizations, decision-making authority may be the sole responsibility of the executive director. In functional work groups, the decision-making authority may be less transparent, so the organization should establish the process for preliminary and final approval of procedures and new protocols. This will be particularly important once staff begin doing the actual work that is part of the Self-Study and Site Visit phases of the accreditation process.
Regardless of the structure chosen to manage the work, the individual responsible for overseeing the accreditation process needs to ensure that work groups and teams routinely provide information and updates to them. Sharing information and progress with the leadership team is a must, especially if the accreditation lead is not a part of said team.
Responsibilities associated with stages of accreditation process
There are six stages in the accreditation process, each with different responsibilities. Below are some salient tasks for which the organization is responsible.
Application & agreement
The application and agreement phase of the process is an opportunity for the organization to assess the cost of accreditation and explore the service standard sections that may be relevant to the programs provided. Once the organization has decided to pursue COA accreditation, the accreditation agreement is signed and the work begins.
Intake
Think of the intake stage as COA’s opportunity to acquire information from the organization on all your programs and locations in which they operate. When highlighting the scope of services at each program, be concise. COA uses this information to determine the appropriate service standard for each program. Do not spend many months in this stage of the process – it will prolong the assignment of service standards. The organization’s Site Visit will not be scheduled until all program documentation has been submitted to COA.
Self-Study
When the organization enters the self-study stage of the accreditation process, all standard sections have been assigned and the due dates for the Preliminary Self-Study and Self-Study have been scheduled, along with the start date for the Site Visit.
During this phase of the accreditation process, the organization should implement the structure for managing the standards review. Work groups should conduct an assessment of its current practices, policies and procedures against the COA standards. A self-assessment helps the organization to know where it needs to prioritize its time and resources.
Site Visit
Once the Self-Study has been submitted, the accreditation work groups should begin compiling documentation to have available during the Site Visit. Reserve a meeting room for the Peer Review team to use while they are onsite for the duration of the Site Visit. All documentation should be clearly labelled by standard section, including the relevant core concept standard. The information the Peer Review team will evaluate can be available in paper or electronic format.
Building and sustaining momentum
If you are following the steps as listed, by now the “why” behind accreditation has already been established. An inventory of the strengths of staff has been conducted, and the process for managing the accreditation work is in place. Now the organization needs to formally roll out this significant initiative and keep staff engaged throughout the entire process.
Set a kick-off date
A kick-off event, such as an all-staff meeting, is a great way to launch the accreditation work. Use this time as an opportunity for the executive director to explain to staff why the organization is pursuing accreditation and why it is valuable. It is an opportunity to inform staff that pursuing accreditation can provide professional development and team building.
Themes and activities
Knowing the “why” behind the organization’s pursuit of accreditation may not be enough for some. For those who are charged with managing the accreditation process, consider ways to make different aspects of the work fun and exciting. Television shows, sports, movies, are all options that may be suitable to connect accreditation work groups. Visual display boards serve as a reminder and can foster healthy competition within the organization.
Final thoughts
The accreditation process can be overwhelming —there are many aspects that need to be managed. Hopefully, your creative juices are flowing with ways to make this organization-wide initiative manageable and fun. Remember, to get others involved, align the work with the strengths of staff and challenge the organization to always strive to be better.
Been through the accreditation process before? Share your thoughts on some things you wish you had known before you started the accreditation process. Recently completed the accreditation process? Let us know some of your pro tips that helped your organization through!
It is no secret that the Council on Accreditation (COA) believes in what we do. We promote best practices and help our organizations to implement them with the aim that clients across the social services field will get the best possible quality of care. By accrediting the entire organization, we ensure that everyone—from human resources to finances to support staff—is working together to carry out that mission.

This is the “why” of organizational accreditation for COA and our accreditees alike. We are all here to do good; following best practices helps us do good in the most effective way possible.
Improving service quality is the most important benefit of organizational accreditation. But from our experience, it is not the only benefit! Every time an organization completes the accreditation process, COA asks about its impact. Several themes have come out of our survey responses.
Organizational accreditation improves operations.
Whole-organization accreditation provides a framework for staff to look at how they fulfill their mission now and discover how they can do so better. The benefits along the way are multifold: more open communication, sound strategic plans, streamlined work systems, better risk management…the list goes on. When an organization looks at itself holistically, it can find the root of any problems and be better equipped to solve them.
!["We have really enjoyed the fact that we are united by the power [of] COA accreditation and by sharing our common mission [of] providing children and families, in a contexual and in a multicultural approach, with the best." -Jorge Alberto Acosta, Founder of Nuevo Amanecer Latino Children's Services](https://static1.squarespace.com/static/5817757515d5dbcebad2b0bc/t/5c758d43f9619ac702a6edb4/1551207752285/Copy+of+Benefits+of+Accreditation+Pull+Quotes+%285%29.png?format=1000w)
94% of COA-accredited organizations agree that accreditation improves organizational learning and knowledge. 82% agree that it improves organizational capacity. COA accreditation has helped some organizations bring themselves back from the brink of bankruptcy; others have used it as a tool to position themselves to become leaders in the field.
Many have expressed that reaccreditation is not an end of itself, but a tool to help them achieve new heights of living their mission. COA is proud to help them do that.
Organizational accreditation boosts marketability.
Organizational accreditation is a professional, 3rd-party recognition that an organization meets the highest standard for both quality service delivery and administrative practices. The effort that an organization goes through to achieve accreditation proves just how much its staff cares about what they do.
This hard work helps organizations stand out among competitors and builds goodwill. 85% of our organizations agree that COA accreditation improves their organization’s marketability. 90% agree that it improves their relationship with external stakeholders. Clients and community alike are looking for signs of quality—accreditation gives them a big one.
Organizational accreditation helps secure funding.

Organizational accreditation verifies that an organization not only does quality work, but also has sound financial, administrative, operational, and oversight practices. This third-party verification can inspire the confidence funders need to support an organization as it continues to grow.
This can help in terms of government funding, as well. COA is recognized in over 300 instances in 50 U.S. states, the District of Columbia, Canada, and China. Our list of recognitions continues to grow, and with it the financial benefit to our accredited organizations. As of December 2018, 70% of our organizations agree that COA accreditation ensures funding.
Organizational accreditation can give staff a sense of fulfillment.
Accreditation encourages organizations to look at themselves frankly and work toward continuous quality improvement. This can allow staff to take a break from their daily grind and appreciate the big picture of their impact. Organizational accreditation also facilitates transparency and open communication, which can increase trust and the feeling that everyone is working as part of one team. Finally, the quest for quality improvement provides staff with new professional opportunities, allowing them to lead the charge toward a brighter future for those they serve.
Almost three quarters of COA-accredited organizations agree that accreditation improves workforce engagement, and over half agree that it improves staff retention. Many of our organizations describe how empowering it is to see the change in mindset that accreditation can bring.
Organizational accreditation holds the team to its goals.

As anyone with a broken New Year’s resolution knows, it is easy to put great plans in place and never carry them out. Accreditation (and reaccreditation!) forces organizations to follow through with those great plans, holding them accountable to be the best they can be.
94% of COA-accredited organizations agree that our whole-organization accreditation improves transparency and accountability. Through it, staff become not only accountable to their clients and stakeholders, but to themselves.
Time and time again, accreditation has proved transformative for our organizations, supporting their mission and allowing them to provide clients with the quality service they deserve. COA is grateful and humbled to be a part of this important process.
Have you experienced other accreditation benefits not listed here? Share them with us in the comments!
SOURCE: All statistics are pulled from 2018 survey data from organizations accredited by the Council on Accreditation (COA).
We are all impacted by government spending and regulations beyond our day-to-day work in human services. Regulations empower us as consumers to make informed decisions about our health and safety. They give us peace of mind as employees, that our employer’s practices will be fair and that public spaces will be clean and meet the necessary standards.
We put faith in our political representatives to advance regulation in order to improve the overall welfare of our society. Over time we observe reactive regulation created to address urgent events, gradual regulation to help move the needle on key issues across a country, and preemptive regulation intended to aid the success of future generations.
Let’s explore the role of government regulations and learn more about their value to human services:
Need drives change
First, let’s discuss a historic example of the need for regulation. In September 1982, 12 year-old Mary Kellerman of Elk Grove Village, Illinois, died after consuming a capsule of extra-strength Tylenol. Within a month six more people in the vicinity would be dead and over 100 million dollars’ worth of Tylenol would be recalled from shelves across the United States. These instances amounted to what would be known as the Chicago Tylenol Murders.
The still unidentified perpetrator was purchasing Tylenol in the Chicago area, adding cyanide to the capsules, and returning them to the store. In turn the store was restocking shelves with the returned product and those that purchased and ingested the Tylenol died within an hour of consumption. Johnson & Johnson, maker of Tylenol, distributed warnings to hospitals and distributors and halted Tylenol production and advertising. Police drove through the streets of Chicago using megaphones to warn residents about the use of Tylenol.
In 1983, in response to the incident, Congress passed the Federal Anti-Tampering Bill, also known as the “Tylenol Bill”. The bill made it a federal offense to maliciously cause or attempt to cause injury or death to any person, or injury to any business’ reputation, by adulterating a food, drug, cosmetic, hazardous substance or other product. It also created a FDA requirement that all medications be sold in packaging with tamper-resistant technology.
In the face of a terrifying public safety situation, urgent government regulation was able to ease fears and create a foundation for the way medication is regulated in the U.S. today.
Regulation and our families
An example of regulatory oversight within the human services field is the passage of the Family First Prevention Services Act (FFPSA) by the U.S. Congress in 2018. It marks the largest reform of child welfare financing that has occurred in the past decade. The goal of the child welfare system is to keep all children and youth safe. The regulatory and spending path to deliver that safety has forever been changed because of this legislation.
Today it would be rare to find a human services professional that does not feel the primary initial goal for child placement is reunification with a parent or family member. Acknowledging that to keep kids safe in the long-term we must support families and alleviate issues that may lead to unsafe conditions/removal is widely accepted as best practice. The passage of FFPSA codifies this practice into law and allows funds to be used for family strengthening/preventative practices in child welfare agencies. This is a shift from exclusively funding out-of-home placement, which somewhat incentivized and eased this type of placement.
Though the enactment of FFPSA is a giant leap forward for the field, requiring some states and agencies to change decades of practices and redefining the way we regulate and implement a government program, the overall goal remains the same: to keep all children and youth safe.
Accreditation, a piece of the regulatory puzzle
Accreditation standards serve as a vehicle to implement and verify best practices. COA accreditation is recognized in over 300 instances across the US and Canada as an indicator of quality. In some cases the journey towards accreditation is due to a mandate, which is when states require that certain types of organizations become accredited. Another motivation for seeking accreditation might be due to deemed status, which is when state licensing bodies allow service providers to provide proof of accreditation in lieu of undergoing certain parts of the licensing process. The practice of states/provinces recognizing accrediting bodies is one way that they implement regulation, oversee services, and work to increase quality of services. We recommend checking out the blog post, Help! I’m Mandated! Now What? Choosing an Accreditor to learn more about navigating this topic.
Over time standards are updated to reflect advances in the field, changes in research and practice, quality indicators, and shifts in government regulation. Throughout an organization’s accreditation cycles they are able to evolve with these changes. Accreditation requires that organizations engage their stakeholders, creating an environment for services to adapt alongside the needs of the community. This relationship between accreditors, regulators, and service organizations builds a foundation for continuous quality improvement for both entities, improving outcomes for the clients served.
Conclusion
Instead of approaching government regulations as just another requirement, step back and imagine how they can assist with meeting your organization’s mission. How can these directives support your long-term goals or bolster best practice? As outlined through these examples, regulation is often born out of necessity. These rules can determine a health outcome, the safety of and access to medication, and the path for a child in foster care. At times regulation might seem like another hoop to jump through but in fact it can be a valuable component to your quality assurance toolkit.

A big thank you to Tristan Keelan of TenEleven Group for this guest post!
The Behavioral Health field is undergoing a data revolution where electronic capture of daily activity is expected to produce reports that demonstrate, among other things, quality. The initial response to this paradigm shift is to have an electronic health record that can capture data, and produce reporting and analytics capabilities that use the data to demonstrate agency effectiveness. While front-end data capture and back-end information reporting are certainly critical elements of the value based care equation, there is still an element of intervention required by your Quality and Compliance staff to ensure that your data has integrity. To achieve data integrity, you need to make sure that you’re collecting your data in a repeatable manner that provides consistent and accurate data.
Find your outcomes measurement tool
One of the best ways to demonstrate value in behavioral health is to adopt standardized outcomes measurement tools. Tools like the CANS/ANSA, PHQ-9, DLA-20, GAD-7, Columbia Suicide Risk Scale, and many others are designed to allow for the measurement of client populations to be viewed in aggregate for the purposes of demonstrating agency effectiveness. However, the integrity of the outcomes data you capture is going to be critical for framing the story telling that is done once your results are in.
3 tips for maintaining outcomes integrity
The three critical elements that you can manipulate to drive data integrity within your outcomes tools all revolve around creating and enforcing repeatable processes. When your processes are repeatable, you can present your reports with foundational context that improves your presentation. This can turn “here are our numbers,” into “We follow these processes and procedures, which we know drive success, and the proof is here in our numbers.” And the second version is much more convincing.
These three elements are:
1. Determine the cadence that outcomes measures will be captured by, and enforce it.
You want to use standardized outcomes measurement tools so that you can find a way to commonly measure success across your patient population as the progress through treatment over time. Normally when we measure patient outcomes over time, we would make the date the tool was administered the X-axis that would drive our visual; however, in the case of behavioral health outcomes measurement at the agency level we cannot do that.
If you were to look at outcomes scores by date, you end up with a mash up of scattered data because clients are not all seen on the same days. For a visual example, look to the PHQ-9 outcomes scores shown in the graph below:

To rectify this and bring your clients into an “apples to apples” view of progress, you must group the scores into the iteration of the form that was administered – first time, second time, third time, etc. When you do that, you bring a focus to what your outcomes look like at the agency level.
The image below shows the same data set, for the same time period, but it is organized with “Administration Number,” as the X-axis to bring the average improvements of client across the agency into focus.

To make this data tell the story you want, you must be able to articulate what your process for capturing the outcomes measurement is. For example, the measure could be administered every time the customer is seen. Or, every 3rd visit. Or, every 3 months (maybe this coincides with treatment plan reviews). Whatever your agency’s choice is, it should be agreed upon, and enforced. From a quality enforcement standpoint, there should be monitoring reports and procedures to follow-up with therapists who have clients fall out of the agency defined outcomes measurement procedures.
Those monitoring reports can also be run historically to determine how often your process is falling outside the desired timeframes, and thus how far off your data integrity is from the desired. If your monitoring reports show that your clinicians are administering the PHQ-9 at different points in treatment for each client, you will have a low data integrity.
Your agency should strive to be able to speak to outcomes in terms of the example phrase, “the positive trend in PHQ-9 scores reflects our process to administer the measurement tool within 14 days of the treatment planning due date, which we achieve 99% of the time.”
When your Behavioral Health agency can add these types of process statements in conjunction with positive trending outcomes reports, then your value proposition appears substantially stronger to your audience.
2. Acknowledge outcome drift – respect the anchors and keep them front and center
Your clinical staff wants their clients to improve; that’s why they got into this business in the first place. However, this presents a common problem for clinical staff who administer scoring tools. Because the desire is for the client to improve, the previous score can often replace the scoring anchors in the subconscious of the person doing the scoring.
For example, consider the following simplistic version of a hypothetical 3 point symptomatic scale.
In the past month, how often did you experience feelings of anxiety?

In our example, let’s assume the client has scored a 2 on the past two administrations of the tool. The therapist can begin to rationalize that while the client is exhibiting signs that reflect a 2 = Some of the Time, they seem to be doing better overall. Instead of marking a 2 for the third time in a row on this question, the therapist can begin to use the desire for improvement to justify marking a 1 = Very Little because of the appearance of overall improvement.
This type of “Anchor Drift” is natural and should not prevent the use of standardized outcomes tools, but rather should be protected against. There can be a tendency in EHR software systems to streamline forms in a way that removes unnecessary elements that may have existed in the original paper version. This is where it helps to combat that tendency to drift toward improvement by making the anchors present on the form every time it is completed.
In this case if our anchors, “Very Little,” “Some of the Time,” and “All of the Time” are right next to the questions, it will help to subconsciously override the client’s previous score as the anchor. Stripping out the anchors on an electronic form seems like an efficiency gain of space on the screen, but a smart EHR will keep outcomes anchors present on the form to hold the integrity of the tool above the well-meaning desire for clients to improve.
3. Periodically audit your outcome tool with self-assessments
In conjunction with the previous effort to maintain integrity to the outcomes anchors, you can enforce an audit of your clinical staff compared against your client population. Introduce the client to the outcomes anchors, and ask them and the therapist to each complete separate versions of the form at the same point in the treatment. Then you can measure the variance between them at the agency, therapist, and client levels.
As with all things discussed thus far, there are multiple ways to conduct this audit, and it’s really all about establishing and maintaining process. You can dictate that a self-assessment audit is performed every fourth administration of the outcomes tool. Or, call for random self-assessment auditing at different points and have the audit reflect a date in time, versus a static stage of the process that moves with time. Both methods demonstrate that the agency is committed to maintaining anchor integrity. If the anchor drift feels strong, the agency can move towards refresher training or other follow-up methods that are meant to always keep therapists scoring to the anchors.
Show off your good work
When presenting data, you want to be able to articulate the procedural steps that your agency is taking to ensure that showing a positive trend line can be taken as a representation of actual client improvement. This can make all the difference between winning a contract or being overlooked despite your good work.

The views, information and opinions expressed herein are those of the author; they do not necessarily reflect those of the Council on Accreditation (COA). COA invites guest authors to contribute to the COA blog due to COA’s confidence in their knowledge on the subject matter and their expertise in their chosen field.

Tristan Keelan
Tristan Keelan is the Marketing Strategist at TenEleven Group. Tristan holds a BA in English from Elmira College and an MBA from St. Bonaventure University. He uses his experiences working in Government, Non-profit National Service, and Banking to bring business process and analytics driven insights to the behavioral health industry.
You can read blog posts from Tristan here.
If someone were to rate their wellness level, their first instinct might be to measure their physical or mental health against common indicators, such as the presence of an illness or injury. These markers are a good place to start, but one’s health status does not happen in a vacuum independent of their environment.
As the United States continues to find its healthcare system under fire, one issue many point to is the health disparities mediated by race, ethnicity, geography, orientation, socioeconomic status, etc. Both level of education and socioeconomic status have direct correlations to health status, with individuals living in poverty eight times as likely to have poor health outcomes. As recently as April 2018, the New York Times reported on significantly high mortality rates for America’s Black mothers and babies in comparison to their white counterparts and how that relates to their lived experience.
Often times your health is influenced by factors beyond the individual’s control, factors related to their social context. Health professionals refer to these as social determinants of health (SDOH) and they have become the focus of increasing interest when it comes to closing the health disparity gap and taking more proactive approaches to population health and well-being.
Defining SDOH
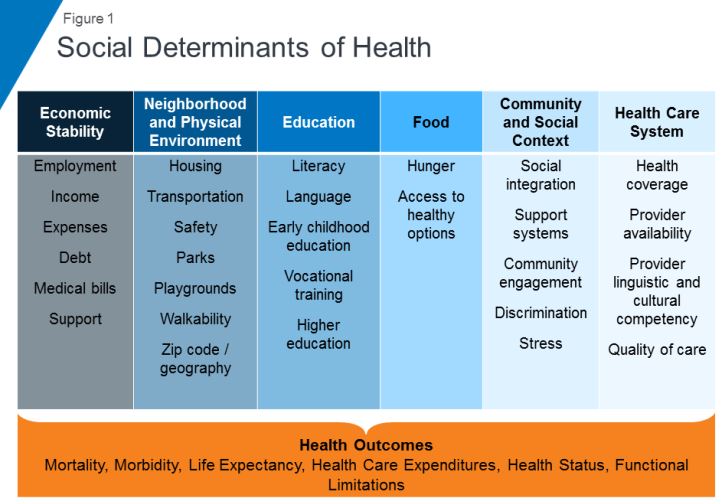
SDOH refer to economic and social conditions and their distribution among the population thus influencing individual and group differences in health status. They are factors found in one’s living and working environments rather than individual risk factors such as behavior or genetics, which can impact one’s vulnerability to disease.
The Center for Disease Control (CDC) and the World Health Organization (WHO) have both emphasized the importance of taking into consideration the conditions in which people live, learn, work, and play when assessing health status. WHO frames the potential for these experiences to be health-damaging as “the result of toxic combination of poor social policies, unfair economic arrangements, and bad politics,” calling for society to look beyond the health sector when dealing with issues of health and disease.
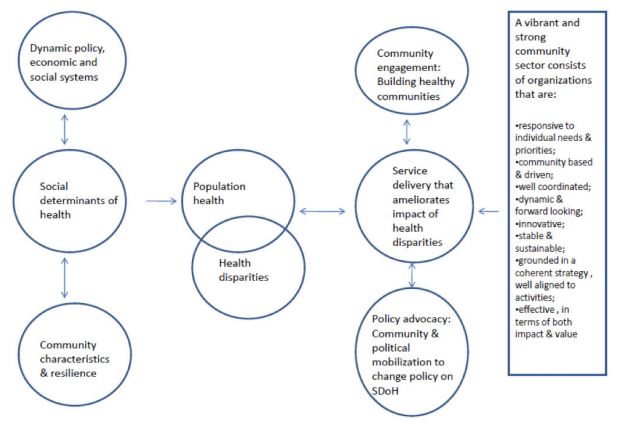
Audrey Danaher, from the Wellesley Institute, created a framework to describe how these social determinants may play upon each other given that the impact is not direct, but mediated. For instance, community characteristics and resilience can have an effect upon SDOH independent of policy, economic, and social systems. A responsive community sector (e.g. non-profit organizations that provide services within communities to meet needs) can help to reduce the disparities through engagement, advocacy, and service delivery. It is worth noting that Danaher’s data and framework comes from communities in Canada, which has universal, single-payer healthcare, further supporting the argument that individual health goes beyond just healthcare.
SDOH on individuals’ health
SDOH play a significant role in individuals’ health outcomes, and research has demonstrated that there is a social patterning of disease. Per Williams, Sternthal, and Wright (2009), “disadvantaged social status predicts higher levels of morbidity for a broad range of conditions in both children and adults.” Growing up in economic poverty in and of itself is correlated with a broad range of health-damaging conditions (e.g., family turmoil, neighborhood violence, consume polluted water and air) and growing up as part of a marginalized community increases your exposure to psychological stressors. But how do these things in turn play a role in individuals’ health?
Let’s look at asthma. While the consumption of polluted water and air increases the risk of asthma within the population, this alone does not fully account for this disparate distribution childhood asthma. In a 2017 study, researchers found that African-American children living in lower socioeconomic neighborhoods were 8.8% more likely to have asthma than their white counterparts, 6.7% more likely in middle-class neighborhoods, and 5.8% more likely in affluent communities. Not only are there differences among racial lines, but youth in more deprived communities are significantly more likely to have asthma emergency department visits and significantly more asthma inpatient admissions. Some SDOH identified as playing a role in these group differences include maternal stress during pregnancy, living in communities with higher levels of violence, overburdened or absent social supports, and psychological morbidity.
Another example of a SDOH is food insecurity, defined by the U.S. Department of Agriculture as a lack of access to enough food for an active, healthy life. Food insecurity is caused by a number of elements such as income and unemployment, disability, and food deserts, which are associated with both socioeconomic status and race/ethnicity. Food insecurity does not necessarily cause hunger, although it is a possible outcome, but it is tied to chronic disease such as hypertension, hyperlipidemia, and diabetes.
Community sector in action! Connecting SDOH to service delivery
Community sector initiatives have often taken the lead in responding to deprivation and negative SDOH. Due to the nebulous nature of SDOH and how they’re specific to different communities and populations, it makes sense that change comes from within the community itself. Just as communities can be a cause for poor SDOH, they can also be the catalyst for improving them and thus improving the community’s outcomes.
Majora Carter’s environmental justice work in the South Bronx is an excellent example of a community-driven response to SDOH. The South Bronx is home to a significant number of industrial plants, including waste processing (40% of the city’s waste and 100% of the Bronx’s end up there), sewage treatment, and four electrical power plants. It has the lowest ratio of parks to residents throughout the entire city; it ticks all the marks on social determinants of health listed above as well as the poor corresponding outcomes. Carter started with the goal of creating a new park, which subsequently led to a greenway movement. One of her next moves was to secure funding for a waterfront esplanade that allowed for a wider range of forms of transportation, thereby influencing policy on traffic safety in the area. Using social capital, she also created facilities that would not only bolster the health of residents in the community but improve quality of life (e.g., encourage residents to be more active) and create opportunities, such as green-collar jobs and community business investment. By recognizing and focusing on the impact of the environment on the health and safety of its inhabitants Carter was able to develop solutions to improve the health of her neighbors.
Carter’s success is not isolated. COA accredited organizations are the community sector and often occupy the spaces needed to rehabilitate SDOH. While this not has always been an explicit or even conscious goal of human and social service delivery, if you look at the SDOH listed in the graphic above, you can map the services provided by COA accredited organizations onto the list. Whether it’s providing youth with alternatives to out-of-school suspension, offering assistance with navigating the healthcare system, or providing housing and community resources in a supported living program, all of these solutions fill gaps in the community and boosts their SDOH.
Next steps
This wouldn’t be a COA blog post without a few ways in which you can get involved. Here are a few initiatives working to improve social determinants of health:
One of the most powerful actions you can take is to get involved with your own community. What are some of the issues you see around you? What are some of the areas that need further support? Are there grants from your city to help implement the changes needed? Chances are, there are already organizations working towards improving community health outcomes with opportunities to volunteer or partner.
In the high-intensity, resource-scarce universe of human services, the service environment itself often gets overlooked, or else overshadowed by compliance concerns. Against the backdrop of serving families at risk, individuals in crisis, and struggling communities, all while trying to keep the doors open, space planning concerns like layout, furnishings, lighting, and décor can seem trivial. Facility design might sound like a luxury, but in reality it has a presence in almost every aspect of service delivery. The evidence is clear. The physical environment can have a profound impact on behavior, mood, perception, and accessibility. When designed intentionally and strategically, your facility can support the work and mission of the organization. Left unexamined, it can limit or even undercut your impact.
Whether you’re opening a new site, considering a relocation, planning a renovation, or just looking for ways to refresh your facility in a way that improves the effectiveness of your services, here are some important issues to consider:
Safe space
The most fundamental concern for every organization is safety. Every facility has to comply with building codes and regulations aimed at protecting occupants from hazardous conditions. Features like emergency exits are specifically designed to promote safety by influencing behavior in the event of a critical incident – such as evacuating during a fire.
Serving vulnerable populations, however, often means preparing for and responding to critical incidents stemming from distress, conflict, and harmful behavior. In recent years suicide prevention has become a focal point for facility planners and is emerging now as a powerful example of how the built environment can be leveraged to save lives. Organizations serving populations at risk for suicide are embracing the imperative to scrutinize all architectural features, fixtures, and materials in the service environment for their potential to become an instrument for harm – specifically as an anchor point or ligature. Shatterproof glass, round-edged doors and tables, breakaway curtain and closet rods, and tamperproof power outlets are just a few examples of features that have been designed to be suicide-resistant. The layout of the service environment can also play a role in reducing opportunities to self-harm; placing staff areas in close proximity to high-risk individuals allows for consistent yet non-intrusive observation.
A trauma-informed approach tells us that identifying and addressing triggers or trauma reminders is key to preventing and de-escalating crisis situations. Organizations must examine both the physical and psychological safety of their facilities and keep in mind that the built environment itself can be a trigger or stressor. An enclosed, restrictive space can often be triggering for individuals with trauma histories or individuals with certain mental disorders, such as schizophrenia; this is often addressed by foregoing corridor layouts and installing glass doors that enable individuals to get a clear view from one service area into the next. Planners also often avoid using the color red to avoid associations with blood, fire, and emergency lights that can trigger a trauma response. Individuals coping with anxiety or PTSD can be overstimulated by patterns, brightly contrasting colors, or other visually complex designs; neutral or softer colors with more subtle transitions are therefore generally more appropriate for therapeutic environments.
While safety is imperative, there are plenty of other ways the built environment intersects with organizational goals and priorities. Now that we’ve looked at how the physical environment can reduce suicide, harmful behaviors, stress, and aggression, we can turn to how it can reinforce and encourage positive behavior and promote better client outcomes.
The client experience
A well-planned facility should complement your organization’s work by ensuring that individuals and families feel safe, supported, and in control while they are receiving services. To learn more about how organizations use the built environment to support their work, we spoke with Children’s Institute, Inc. (CII) in Los Angeles, a COA-accredited organization that provides a broad array of mental health, early care and education, child welfare, family support, and youth development services to children and families – who are also currently in the process of relocating one of their sites and constructing a new campus.
A client-centered approach informs many of the crucial decisions CII has made in identifying and designing their new facilities. “We thought about how it would affect the client’s experience, being on one floors or two,” says COO/CFO Eugene Straub. CII has been careful to ensure that their facilities are welcoming to both clients and staff. “The goal is building a sense of trust and security. The last thing you want to do is make anyone feel uneasy.” Improvements have also been made to existing sites where the space was not meeting families’ needs. “We had a nice lobby and waiting areas but there were no activities, and we looked for ways to change that and make the space more inviting and inspiring.” Now CII’s once-empty waiting areas include a lending library and creative space for children and families to use.
What are some ways that your organization could find inspiration and ideas when planning facilities? Your service recipients, staff and community are a great resource for ideas and a great place to start. Organizations should always look to their service recipients and their communities for ways to enhance their service environment, and tailor their facilities to the unique needs of the service population and to their service model. For example, a residential facility for individuals with schizophrenia can provide some relief to residents coping with paranoia by orienting beds and desks to face the door. A youth development program for children with autism spectrum disorder, who often struggle with spatial navigation and wayfinding, should consider applying visual cues to transitional spaces. Every organization’s approach to designing an effective and supportive service environment will be unique and depend on their scope, service population, service model, and culture. But there are a few universal design features that facility designers and environmental psychologists agree contribute to a calming, welcoming, and therapeutic service environment:
Nature equals nurture
Studies have consistently shown that access to nature, whether physical or visual, has a calming effect. Treatment facilities often situate themselves in a natural setting for this reason, but any organization can look to existing assets to bring to their full potential, such as a small outdoor space that can be converted into a courtyard or garden, or installing windows to take advantage of a good view. Organizations that are truly limited can still make enhancements by incorporating plant life into the decor and displaying nature and landscape art, which have also been demonstrated to have a positive and calming effect on mood.
Let the sun shine
Sunlight triggers the release of serotonin, which boosts mood and focus. Research also indicates that the ability to identify time of day through observed sunlight is conducive to re-establishing perception and natural thinking while minimizing disorientation. Natural light also makes small spaces appear larger and more open than they are. Organizations should ensure that they’re maximizing and not obstructing their natural light, such as by moving furniture away from the windows, using window coverings that filter rather than block out sunlight, and opening up any doors and windows that would allow natural light to pass through the facility. Transom lights (windows built into the space above a door) and skylights are also examples of architectural features that maximize sunlight while still preserving privacy.
Power to the people
A client-centered and trauma-informed approach to services stresses the importance of giving service recipients opportunities to have a voice in their service plan and at each stage of service delivery. For survivors and individuals coping with past trauma, opportunities to take control and make their own choices are important exercises in self-empowerment and essential steps on the road to recovery. Current best practice regarding residential facilities stipulates that residents should already be encouraged to personalize and decorate their own space. However, when possible, personal choice should also be extended to the environment by giving service recipients the power to customize lighting, temperature, acoustics, or furniture arrangements. To balance flexibility with safety, facility planners often choose furniture that is too heavy to be thrown or used as a weapon, but that can still be moved around and reconfigured, which gives individuals (or groups, in communal settings) autonomy to situate themselves where they feel safest.
No place like home
Experts typically agree that a safe, therapeutic, non-institutional and homelike environment is the best setting for residential treatment. Some strategies that designers employ to make a facility more warm and inviting include using upholstered rather than hard furnishings to invoke a softer, cozier feel, and mixing and matching a cohesive array of furnishings to avoid a uniform, institutional look. Given that “home” is a cultural construct, cultural competency is vital to ensuring that your environment meets the definition of “homelike” for your service population.
Of course, “home” is about more than just furniture — it’s also about people. When designing or evaluating a facility, organizations must consider not only the service recipient, but their support network. Because an engaged and committed support network is one of the most important contributing factors to positive client outcomes, service environments need to promote and facilitate their ongoing involvement. Organizations should be mindful that an imposing service environment can discourage or inhibit the service recipient’s support network, and evaluate whether their facility accommodates and encourages visiting family and friends as well as any collaborating service providers. Is it intimidating for visitors to access or navigate the facility? Are there welcoming spaces for residents to spend time with their visitors, or to have private conversations?
Supporting your staff
Getting your space to work for your service recipients also means ensuring that it works for your workers. As with service recipients, the environment influences workers’ behavior, mood, and functioning – which in turn impact performance and productivity, and your organization’s effectiveness. In human services, an ineffective environment undermines not only your bottom line but your mission.
The human services field also faces significant workforce challenges – namely recruitment, retention, and secondary trauma. Qualified workers are in short supply, in no small part due to poor funding and stigmatization of the service population. Staff shortages and the difficult nature of the work, which often manifests as secondary or vicarious trauma, lead to burnout and to high rates of turnover. Finally, worker turnover negatively affects client outcomes.
These workforce challenges have been at the center of the design and planning process for Children’s Institute, Inc.’s new offices. With the aim of promoting collaboration and “addressing the adverse effects of the work itself”, CII decided to eliminate cubicles in favor of a communal, team-driven open plan layout that will allow staff to support one another, celebrate their successes together, and foster staff resiliency. Straub observed that the cubicle layout often forces staff “to go from meeting with clients to sitting at their desk by themselves” and process their experiences in isolation. The intent of the new layout is to encourage workers to “have more of a shared experience and focus on wellness and self-care both individually and with each other”. The new offices also feature “decompression zones” – calming work-free spaces for staff to recover, including through meditation and yoga, as well as larger common areas, kitchens, and breakrooms. Evolving workplace norms mean that “the younger workforce wants an office space that fosters support and feels less corporate and more collaborative,” Straub explains, making these amenities not just “perks”, but rather, vital resources that will promote staff wellness and strengthen recruitment of valuable staff.
CII is also allocating space for “drop-in” staff – workers from other sites who are out in the field will be able to use nearby CII offices as a landing spot in between client visits. Straub envisions that this increased “cohabitation” will stimulate knowledge and resource-sharing and enhance linkages for families and continue to build the culture of the agency. Emphasizing the importance of “collaborating with the end user,” CII has also been careful to engage staff in the facility planning process, bringing all staff to tour the new space before signing the lease and soliciting feedback about the environment as part of annual employee surveys. Continuous assessment of a new or revamped workspace is not just good quality improvement practice, it also ensures that the organization identifies and addresses any unforeseen effect on employee functioning. For example, in an evaluation study of behavioral health facilities, researchers discovered that staff in a new facility that had been designed to promote client-staff engagement were experiencing greater burnout in response to the increase in client interactions.
Strategic plans to building plans
Creating a safe, effective, and supportive service environment requires the organization to approach the physical environment as part of its mission. It calls for not only commitment and investment, but also a shift in attitude — away from “being happy just to get the space”, as Straub says, and towards leveraging the space to influence how the organization’s operations are experienced and perceived. By tying together their facilities, mission, and strategic plan, CII’s ambitious expansion project received enthusiastic support from its board and funders. Straub sees the new campus as “an opportunity to create organic change” by leveraging the space to build partnerships with the community; plans are already underway to co-locate with other providers and host community taskforces and other grassroots organizing initiatives.
As much as we’d like the primary takeaway here to be “good facility design is not about aesthetics”, it bears noting that a well-designed facility achieves through its appearance two invaluable objectives: firstly, it destigmatizes the organization’s services and service recipients, and secondly, illustrates the depth of the organization’s commitment to the community.
Tell us in the comments: How has your organization used its facilities to support service recipients and staff? What would you change about your current service environment?
Further reading
Building Better Behavioral Health Care Facilities
Rethinking Behavioral Health Center Design
Designing for Post-Traumatic Understanding
6 Behavioral Health Design Trends
Can a Frank Gehry design help change the dynamic of Watts?
Thank you to Tiffany Langston of the Nonprofit Finance Fund for this guest post!

History of the survey
In 2008, the economic downturn created an atmosphere of fear and uncertainty, not just for individuals, families, small businesses, and corporations, but it was also a very scary time for nonprofits and their clients. At Nonprofit Finance Fund (NFF), we wanted to find a way to tailor our financing and consulting services to be the most helpful to charitable organizations. How could we offer support, tools, and resources, so that nonprofits could navigate this tricky time? We decided to ask nonprofits how the changes in the economy affected their bottom line and the ability to serve their communities. The State of the Nonprofit Sector Survey was born.

Nonprofits are a linchpin in creating social good. Yet there is precious little collective, real-time data on how nonprofits are doing. Are they serving more clients or fewer? Do they have the resources they need to do their work? Are they opening new offices, or dangerously close to closing their doors?
We launched the first Survey in early 2009, with little fanfare and almost no promotion. We rolled up our sleeves, opened our rolodexes, and asked our networks to spend 15 minutes to tell us how they were feeling, what they were doing to combat the recession, and how NFF could help them deliver on their missions. We heard from 986 respondents, many of whom told us that they were feeling financially vulnerable, bracing for funding cuts across the board, preparing to end the year with a deficit, and developing a ‘worst-case scenario’ contingency plan. The recession brought into focus a serious, long-standing issue: the nonprofit sector is continually forced to do more with less, and the margin between stability and crisis is often precariously razor-thin.
But the thing that surprised us most was the numerous requests we got from media, researchers, policymakers, nonprofits, and funders, to do a deeper dive into the data. The results were published in The New York Times, CNN.com, and The Chronicle of Philanthropy. There was a thirst for real-time data, and at the time, no one else was doing this type of survey on a national scale.
Over the years, the questions adapted as the sector changed. It became a widely-watched barometer of US nonprofits’ programmatic, operational, and financial health. In 2010, we found that while the economy was recovering from the recession, nonprofits were not having the same success. By 2011, 87 percent of the 1,935 respondents said they still felt like the recession hadn’t ended. In 2012, we started asking about government grants and contracts, and if nonprofits were getting paid on time. The outlook finally started to improve by 2013, and we inquired about how organizations collected data and measured impact. And this year, we asked nonprofits about the diversity of their senior leadership and board members, and if their organizations proactively address racial inequity.
State of the nonprofit sector survey 2018
We are living in volatile times. As we prepared for the 2018 Survey, we were excited to get the pulse of the US nonprofit sector and better understand the challenges organizations now face. The 2018 State of the Nonprofit Sector Survey opened on January 16 and closed on February 28. We heard from 3,369 leaders across all 50 states and a wide range of sizes and missions. Respondents said they’re facing chronic challenges and real-time concerns, remain resilient and committed, but are worried about the vulnerable people they serve.
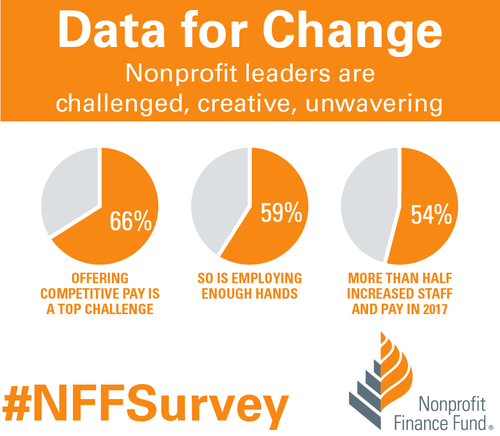
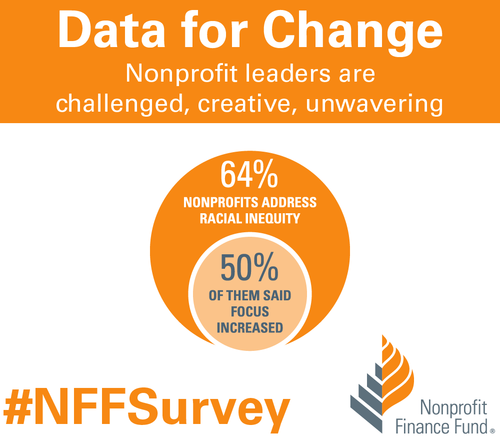
When asked about 2017, 79 percent of respondents saw an increase in demand for services, and 86 percent anticipate an increase in the coming year. Not only did 57 percent of nonprofits find it difficult to keep up with the rising demand last year, but that number swells to 65 percent for organizations serving low-income communities. Despite the challenges, nonprofits continue to invest in programs, staff, and strategies. We found that 52 percent of respondents said their organizations expanded services in 2017, and 63 percent plan to do so in 2018. We learned that 54 percent of responding nonprofits increased staff and 55 percent increased compensation in 2017. We found that 64 percent said they address racial inequity, and half of those said that focus grew in 2017. We also learned that 76 percent of responding nonprofits finished 2017 at break-even or better.
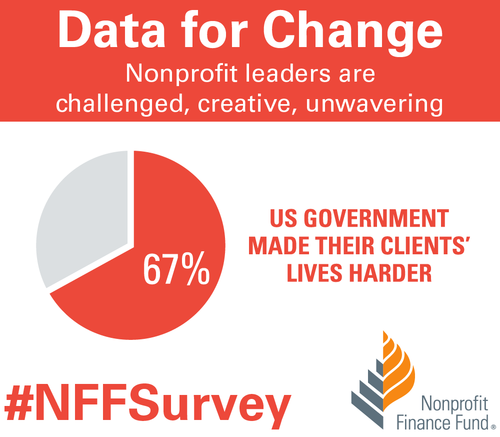
Affordable housing was the most-cited critical community need, followed by youth programs, mental and behavioral health services, and financial capability. We also asked nonprofit leaders how the federal government’s policies & positions influenced the communities they serve, and 67 percent said those practices make their clients’ lives more difficult. Additionally, 37 percent of respondents said their organizations plan to formally engage in policy/advocacy in 2018.

How to use the data
At NFF, our mission is to create a more just and vibrant society. One of the ways we work toward that is by sharing accessible insights, so that the sector has the necessary data to make informed decisions. You can explore the Survey results completely free of charge using our Analyzer. Compare your nonprofit to peer organizations across focus areas, sizes, and geographies. Use the findings to inform planning around strategy and budgeting. Cite data in your campaigns, white papers, testimonials, and grant proposals. Use the data as evidence to support open discussions with funders about the full costs of service delivery and meeting the needs of your communities.
We invite you to dig into the data. Use the filter or combination of filters that gives you the right slice of information for your presentation, board meeting, or application. You can even download images of the visualizations and drop them right into a slideshow or report. Please let us know how you’re using the findings to deliver on your mission. Email us, or share on social media using the hashtag #NFFSurvey. Thank you to everyone who took the State of the Nonprofit Sector Survey, entrusted NFF to raise your voices, and contributed to this critical social sector data set.
The views, information and opinions expressed herein are those of the author; they do not necessarily reflect those of the Council on Accreditation (COA). COA invites guest authors to contribute to the COA blog due to COA’s confidence in their knowledge on the subject matter and their expertise in their chosen field.

Tiffany Langston
Tiffany Langston is the Associate Director, Knowledge & Communications at Nonprofit Finance Fund. She has worked at the intersection of nonprofits and philanthropy for nearly a decade, including overseeing digital communication efforts for WaterAid America and Philanthropy New York, respectively. She is a food lover, writer, and her work has been nominated for a James Beard Foundation Journalism Award.
The social and human services field might conjure images of social workers seeing clients all day in their offices or case managers out on home visits, and although these are aspects of many jobs in this field, the day-to-day reality is often a bit more varied. Social service organizations include a wide array of roles such as human resource directors, finance managers, quality improvement specialists to name a few. And even for clinicians or those in direct practice a good amount of time is spent completing paperwork and other administrative tasks. While these are critical functions of our organizations, those tasks might not be what first attracted us to the social services field. Often, the pull to work in this field comes out of a desire to “give back” or “do good”. And while all tasks in our organizations help to advance the important missions that we signed on for, some of us may still be looking for more or different ways to give back. Many of us might already volunteer for nonprofit boards, give to charity, or volunteer our skills more directly on our own time. Creating or participating in a volunteer initiative in the workplace might assist with scratching an altruistic itch and benefit our organizations at the same time.
You may have heard of the terms corporate social responsibility or corporate philanthropy and thought they weren’t relevant to your organization. The first instinct might be “Our whole function is to create social impact driven by our mission. We don’t need to/have time for/have the energy for additional volunteer work”. You might be surprised to discover that there are still opportunities and interest at your organization to incorporate the essence of these ideas. Specifically, one way is to create a space for employees to give back through volunteer initiatives. After reading on, I hope you’ll find that there are various ways in which doing so can positively reverberate through your work environment, from boosting morale to encouraging closer work with the community you serve.
What are the benefits?
I think it’s hard to overstate the benefits of creating a space for employee volunteerism. For fun, let’s frame it in the context of some COA standards. After all the standards outline best practice!
Human Resources (HR) and Personnel Development and Training (TS)
Staff satisfaction and retention is an area that challenges many organizations in our field. Creating workplace initiatives that keep staff connected to each other and the organization’s mission is one way to help address this. Employee volunteerism initiatives can be a great benefit or perk to highlight for recruiting purposes and to raise morale for current staff. It might be challenging to increase pay or vacation time, but maybe your organization can consider allowing employees time for volunteer activities.
The opportunity to volunteer as a team, department or organization also serves as an opportunity for team building, or dare I say “bonding”. Getting outside the walls of your office and the routine of your day-to-day can allow you to get to know your co-workers in a new light and increase cross-departmental collaboration and relationships.
It also provides an opportunity to develop and demonstrate skills that you might not otherwise have occasion to use while at work. Participating in something different than typical day to day activities can allow opportunities for a newer or more junior staff member to shine in their leadership skills if given the opportunity. Staff might also have an opportunity to develop skills while volunteering. Maybe you can even consider sponsoring an external volunteer organization to come in to train your staff. Some organizations here in New York City require a one-day training in order to volunteer with them. If staff are able to get that training together and through work, it opens up the opportunity for them to volunteer together or on their own.
Community involvement (GOV / AFM)
Another great benefit of volunteering in your local community is the opportunity for community involvement and creating perhaps unexpected partnerships that raise awareness of your mission and presence in the community. You aren’t doing this for PR, but often increased community connections and awareness of your brand is an added benefit. If you have tee-shirts or hats with your branding, and it feels appropriate, you can ask staff to wear them while volunteering to build name recognition.
An event that takes place outside of normal work hours but can be a great opportunity for staff to come together is participating in a walk or fundraiser. Perhaps your organization sponsors a team for a charity walk and then gets outside together on a weekend to participate. Maybe your nonprofit can even offer to trade with another nonprofit and partner to volunteer for each other one day a year. You never know what unexpected relationships can be born out of volunteerism.
One other outside the box idea is if your organization sponsors conferences or events, can you incorporate an aspect of giving back? Maybe an optional day tagged onto the end of a conference for a volunteer activity?
Performance Quality Improvement (PQI)
Lastly, of course – this is COA – we have to tie it to PQI! One way you might consider looking at creating volunteer opportunities at your organization is to incorporate it into your PQI initiatives. If staff express interest, this absolutely works in relation to any of the areas listed above and tied into goals around staff retention, community awareness, or cross-departmental collaboration, for example.
Show me the data
Speaking of PQI, of course in this day and age, you want your decisions to be supported by stats and data. Well, lucky for you, we’ve got it:
- A 2017 Deloitte Volunteerism Survey of working Americans found that 88% of respondents believed that companies who sponsor volunteer activities offer a better overall working environment than those who do not.
- Research from the University of Georgia, supports the fact that employee volunteering is linked to greater workplace productivity.
- America’s Charities Snapshot 2017, is a great resource for data related to “What U.S. Employees Think About Workplace Giving, Volunteering, and CSR”. Their CEO Jim Star, states “Employers who build programs that connect workers to each other, expose them to corporate leaders, and give them meaningful ways to make a difference in their communities send a strong statement to those workers that they are valued. They also build stronger teams and deeper relationships.”
- COA’s nonscientific staff survey showed similar results: When asked to share what they liked best about COA volunteer opportunities, 88% indicated that it “promotes team-building and builds camaraderie.”
COA – Practice what you preach
Here in lower Manhattan at the COA offices, we think this is one area where we definitely walk the walk. After Hurricane Sandy hit the East Coast and New York City hard in 2012, COA staffers spent a day on Staten Island cleaning out a home affected by the storm. Even for those of us in New York who lived through it, the impact of seeing the devastation to that part of the city was sobering. It also was a wakeup call that we as staff were eager to give back outside of our day to day work, and appreciated the opportunity to get out of the office, roll our sleeves up, and interact with our community. After that event, staff expressed (through our staff suggestion box!) that COA should formalize an employee volunteer initiative. The COA Volunteer Committee was born out of this experience.
To date, thanks to dedicated staff and support from COA leadership, the COA Volunteer Committee has been up and running for over five years. Highlights include reading stories to kids, chaperoning an urban garden project, cleaning up Governors Island, shucking corn for a food bank, lending our hands for a meal delivery organization, donating to coat and backpack drives, and more.
The internal response to these initiatives has been overwhelmingly positive. On staff surveys, we’ve heard feedback like “The volunteer activities promote team-building, a sense of community and positively contribute to staff morale”, “generates collaboration” and, our favorite – it gives “the warm fuzzies”.
Helpful tips
To leave you with some tips from our experience:
- Get buy-in from the top: As with many things, buy-in is key. Leadership endorsing and participating is a key factor in your volunteer efforts success. Lead by example.
- Staff input: Before you make a decision about your volunteer activities, it helps to get a sense of what people are interested in. You might create a simple staff survey to get input and specific suggestions, and then figure out what is the best fit for your audience.
- Variety: If you work for an organization focusing on children, maybe one year you volunteer to plant trees or weed a community garden. If you work in adult substance use, maybe arrange to spend an afternoon reading to kids.
- Risk prevention: You’ll want to consider any risks that may be associated with the planned activity and take steps to mitigate those risks. Setting some simple but clear guidelines for participants is a good way to make sure everyone has clear, shared expectations. A few you might think to include are dress code expectations, time commitment, meeting spots, and communication protocols for off-site, to ensure everyone is on the same page from the start.
- Closing the loop!: A post-activity survey or debriefing to capture what people liked and didn’t like about the activity (or for those who didn’t, what hampered their participation), can give you great insight into what to look for next time.
In the end, only kindness matters
Clearly, there isn’t a one-size-fits-all approach when it comes to volunteer initiatives for social and human service organizations. What works at one organization, might not be a fit at another. However, based on the data, as well as our experience at COA, I encourage you to give some thought and get creative about how this might look for your organization. Maybe start small with just your team or department sponsoring a coat drive this year. Or, some of you may already have robust volunteer initiatives in full swing at your organizations. We’d love to hear about workplace volunteer efforts you may have participated in or put into place at your organization. Please share any questions, thoughts or success stories below!
A big thank you to Leslie Chaplin for this guest post!
Making the shift from therapist to administrator can be tough. Being an effective leader is not the same as being a great therapist and many of us get promoted without any formal training in leadership.
With the help of my organization, I am completing a PhD program in Organizational Leadership at The Chicago School of Professional Psychology. Deciding on a dissertation topic was a process of considering what our field could most use in terms of children’s mental health and also in terms of leadership. As our profession has become better at trauma-informed care we have done an excellent job at educating and preparing our staff for the phenomenon of vicarious trauma. However, I have seen a mindset develop where the risk of vicarious trauma becomes such a strong focus that it almost becomes a self-fulfilling prophecy. Leadership responds by communicating about self-care and work life balance. I began asking myself, if our work is so traumatizing, then why would anyone do it? The answer is vicarious resilience, the topic of my dissertation.
Vicarious trauma and vicarious resilience
Vicarious trauma is a term that can be somewhat interchangeable with things like burnout or secondary traumatic stress. It materializes as we listen to the stories of clients who have known horror, unspeakable fear or near death experiences. As we hear these stories over and over the risk of showing the symptoms of trauma become very real.
Vicarious trauma is deeply ingrained in our dialogue and training to mental health professionals, and staff is quick to fulfill our predictions. We address vicarious trauma by urging staff to focus on self-care – things like taking vacation days and exercising. This may provide temporary relief but it does little to reduce the trauma felt once returning to work. I have supervised many brand new therapists in the trauma field and they are always eager to make a difference and help the kids through the tough things that have happened in their lives. We train them for what they will likely experience and the personal struggles that will come with the job of trauma professional. This is important, however, it can become a primary topic of conversation with both the supervisor and the therapist becoming overly focused on the trauma. The point of healthy awareness often becomes overwhelmed by the perseveration and anxiety about traumatic experiences. Taking time away from the job is often where the “self-care” plans end. If we, as leaders in the mental health field, want to reduce our staff turnover and keep our trauma therapists healthy and thriving, we need to do more than grant vacation days.
Where we are falling short is completing the cycle of trauma work and neglecting a critical piece of the process which leads our staff to heal and makes our difficult work worthwhile: vicarious resilience. Vicarious resilience happens when the professional experiences personal growth in their own life through witnessing the growth of their clients.
The concept of Vicarious Resilience was first defined by Hernandez, Gangsei, & Engstrom (2007). Their grounded theory study examined the experience of psychotherapists working with victims and families of political violence. They found that witnessing their clients overcome adversity demonstrating an immense capacity to heal had a positive effect on the therapist. The therapists’ own attitudes and emotions were changed allowing them to reassess their own problems and were better able to cope with their own adversity. The main finding for trauma professionals is their work does have a positive effect on the therapists, and this effect can be strengthened by bringing conscious attention to it (Hernandez, Gangsei & Engstrom, 2007).
Those of us who have been in the field for decades and still love coming to work every day do it because we experience vicarious resilience. Resilience is succeeding against all odds; it’s overcoming adversity and having the grit within you to rise above what is trying to keep you down. As the client taps into their resilience with the help of the professional they begin to get better and as a result the professional shares in the process of getting better. A therapist who can fully embrace this phase of the process will find themselves becoming stronger and more resilient in their own lives leading to higher job satisfaction, less burnout and less turnover in employees.
Harnessing the power of resilience
Research shows that by simply talking about the concept of vicarious resilience and letting people know that it exists (just like we do with vicarious trauma) will raise the likelihood of people having the experience. I have found (in research and in practice) that adding resilience to the conversation brings an immediate shift to the dialogue. We develop insight into our own response to the trauma work and then shift to the successful moments where healing is starting to develop. When the professional can maintain a focus on what has been accomplished instead of the struggle that remains, they create a sense of purpose, fulfillment, and motivation within themselves to stay in the profession. This leads to successful cases of healing and resilience in the child, giving the professional more opportunity to experience vicarious resilience within themselves. In the end, it’s really a simple concept. Stay positive! But in practice, it is predominantly missed and overlooked.
My training on vicarious resilience resonated with Faith, a Northwood residential counselor, who reflected,“Our jobs are hard sometimes and we forget to focus on the success stories. Learning about Vicarious Resilience immediately turned my mood around and I felt like a weight was lifted off my shoulders”.
As leaders, we need to support our staff by helping them realize that self-care does not mean take time off of work only to come back to these traumatizing clients. Self-care should focus on resilience including taking time to play, have fun and notice the positive steps. Look for the successes, no matter how small. Focus on the struggles that have been overcome in the past. Identify strengths and potential. Know that anything is possible and healing really does happen. Use inspirational photographs or phrases that focus on resilience. Remind yourself of the greater purpose in what you are doing. Find encouragement in a smile, a laugh. I’ve found incorporating these success stores into my everyday interactions with colleagues and staff is an effective way to reinforce this as a concept. At your next case record review or team meeting, in addition to focusing on the usual questions, you might try asking staff to tell you about a success from the past year. Connecting a tangible, specific example to the concept of vicarious resilience helps reinforce the power of what could otherwise be abstract. When I did this recently, one of my staff recalled a client recently sharing that she had taught him how to smile again. That is a powerful example to call upon and connect to the concept of vicarious resilience. Following up on those moments of resiliency 3 months later and taking the time to check in on the successes can make all the difference. Remember “this too shall pass” (Persian adage) and “what doesn’t kill you makes you stronger” (philosopher Friedrich Nietzsche). Make a difference in the clients’ lives and help them find their resilience because that is how you find yours. If we are asking our clients to get out bed each morning in the face of their challenges, we realize we need to be, and are, able to do the same. They get better, we get better.
We stress personal resilience in our therapeutic models for our clients and it’s time to start stressing it with our staff. Mental health professionals undoubtedly see resilience in their clients. To be a child who has experienced significant trauma and come out on the other side takes significant strength and resilience. We see the resilience in them, and it makes us better people. This is why we do the work that we do. We absorb the strength we see in them each day and we are able to incorporate it into our own lives – in our work, with clients and with others. The impact is exponential.
It’s an exciting time for vicarious resilience as we begin to recognize and name it in our work. If this concept resonates with you in your personal and professional experience, we’d love to hear about it in the comments below!
Reference
Hernandez, P., Gangsei, D., & Engstrom, D. (2007). Vicarious Resilience: A New Concept in Work with Those Who Survive Trauma. Family Process, 46(2), 229-241 13p
The views, information and opinions expressed herein are those of the author; they do not necessarily reflect those of the Council on Accreditation (COA). COA invites guest authors to contribute to the COA blog due to COA’s confidence in their knowledge on the subject matter and their expertise in their chosen field.

Leslie Chaplin
Leslie Chaplin has over 20 years of experience in the field of children’s mental health including work as a director, child/adolescent psychotherapist, clinical supervisor, program consultant, school social worker and adjunct instructor. She holds a Masters degree in clinical social work from the University of Minnesota and is a PhD candidate at The Chicago School of Professional Psychology. Her passion is the development of new programming to better serve children with mental health needs across disciplines and leading change to better organizations. She is a proud member of the Northwood Children’s Services Executive team in Duluth MN where children and families have been served for over 130 years. Leslie is currently a Peer Reviewer with COA and actively researching the phenomenon of vicarious resilience. When not at work she is happily working on her hobby farm and training therapy animals.