A big thank you to Ruben Mina, LMSW for this guest post!
Can you tell me the history of your community?
Can you tell me some histories of your community?
Yes, histories.
Do you ever ask these questions of adolescents with whom you work? There is a distinction between the two questions. The first question focuses on one story: the prevailing story of how a community came to be what it is. It feels like asking adolescents to pull something in from the past, make sense of it and connect to it.
The second question asks adolescents to tell histories of their community. It invites them to share the who, what, how, and why about the people, institutions, political forces, cultures, and much more that make their community dynamic. Like adults, adolescents have a range of experiences in the communities to which they belong that are rooted in traditions they observe, inequities or injustices they endure or witness, and forms of oppression about which they are aware. They deserve the space to tell their stories. Each individual experiences and interprets life in their community in ways that cannot, and should not, be captured by a single history. By creating space for adolescents to share their varied perspectives and experiences, we are supporting their social and emotional development.
This is not about adolescents being unable to make sense of standard accounts of history. Nor is it about making up stories. It is about engaging adolescents in critical thinking and critical dialogue so that the histories they see, feel, and live each day are amplified. This deepens their connectedness to their respective communities, cultivates empathy, and provides a foundation for them to work collectively to transform their communities.
Mapping histories
While both questions at the beginning of this blog post could create opportunities for shared learning, focusing on multiple histories of a community does more. It invites adolescents to further develop self-efficacy by telling and showing one another the ways they view the world around them. Youth-serving programs want to build adolescents’ sense of self-efficacy, while letting them know that their voices matter. We let them know their voices matter when the learning that happens in human service organizations honors their perspectives.
Earlier in my career, I developed a group activity called “Community Stories” as a way to center adolescents’ experiences, while facilitating their exploration of ways they could transform their communities. This activity has helped adolescents in the Bronx in grade levels ranging from upper elementary school to high school identify and raise awareness about issues such as domestic violence and a lack of neighborhood parks that were impacting their daily lives.
Community Stories take the form of maps that reflect adolescents’ insights about experiences they have in a community to which they belong. It integrates numerous concepts and approaches, including: popular education concepts (participatory, group-oriented), photovoice, and community asset mapping, as well as literacy-building activities. The maps require basic art supplies and no art skills; they are animated by the dialogue adolescents engage in about the ways a group 1) experiences a shared community and 2) envisions its transformation.
This activity allows adolescents to explore a community they identify with in creative, empowering ways, and is intended to engage them in a communal exercise. Constructing maps to tell community stories allows adolescents to reimagine their communities and envision their transformation. By trusting and engaging the expert wisdom of adolescents’ lived experiences, you are letting them know that you value their agency.
Before creating maps, the group must identify a community to which they feel connected and would like to represent on a map. Since communities are not strictly defined by physical borders, it is vital to encourage consideration of non-geographic communities (i.e. community of teen activists). This is crucial for two reasons. First, adolescents are in the developmental stage of exploring membership in groups based on interest, values, and identity, not solely geography. Secondly, this allows for greater inclusivity, particularly for adolescents who experience oppression or marginalization as a result of others’ targeting them based on identity or perceived identity.
These maps are populated by what I have termed “characters” (feel free to use different terminology). “Characters” are representations of those elements that impact adolescents the most (i.e. institutions, places, events, policies). As a facilitator, I have found it helpful at this stage to engage adolescents in naming the dynamic relationships between people and other elements of a community and the meanings of such relationships.
Below is a description of the activity, with facilitator instructions.
Creating the maps
Benefits of the activity:
- Build community around shared experiences of oppression and/or shared visions of transformation
- Promote critical thinking and critical dialogue
- Identify dynamics that impact adolescents’ lives, while encouraging their self-advocacy
Framing questions to ask at the beginning, and revisit throughout to encourage dialogue:
- What comes to mind when you think of the word ‘community’?
- What do communities consist of?
- How can we understand a community?
- Are people the only entities that have stories to tell about the communities we belong to?
Step #1 – Map design
Ask participants to name a community they belong to and want to transform and/or take action in response to an inequity and/or oppression that has been individually or collectively experienced. Instruct the group to create a map that features “characters” (i.e. places, buildings, institutions, policies, rules) that comprise their community (geographical or non-geographical). Pay attention to group dynamics to ensure an equity of voices in the decisions of what gets placed on the map. For non-geographical communities, participants could use systems, policies, and/or institutions as “characters” that impact the community. Relationships and power dynamics can be shown by giving “characters” different sizes (i.e. the bank is the biggest thing on the map because of its impact on the community’s economic state).
Step #2 – Mapping the story
Introduce the word balloon for dialogue between “characters” on the map and thought bubble to see the inner thoughts of a given “character”, and explain their purposes.
Present the reflection questions below and instruct participants to use word balloons and thought bubbles to represent dialogue between the “characters” about the transformation or oppression that was identified in step #1. Reflective questions may include:
- What would each “character” say about its experience with, or observations about, the oppression or vision of transformation that was identified?
- What observations has each “character” made about the oppression or vision of transformation?
- If we could read the thoughts of each “character,” what would we learn?
Participants should then discuss the questions or other questions that may resonate with the group and write responses on the word balloons and thought bubbles. Participants can then place the shapes on the corresponding “characters” on the map.
Step #3 – Expanding the story
Introduce two tools (adapted versions of “flashback, flash-forward” and “hot-seat the character”) that the group will use to engage in critical dialogue. Prompt the group to think about what the “characters” would say if they could flashback or flash-forward in time. For example, if a park is represented on the map, a flashback question could be: what would this park have said was its experience with gentrification 10 years ago?
Next, invite a group member to “hot-seat” another “character”. Group members then get to pose questions to the “character” that are discussed as a group. The focus can be on expanding upon what was written in the word balloons/thoughts bubbles, or what was shared in the flashback and flash forward discussions. For example, a group member might “hot-seat” a group mate’s school “character” and ask: why do you want school administrators to do more to make families feel welcome in the school? Such a question, and others, could engage the group in deeper discussions about school-community relationships.
Step #4 – Processing, closing, action steps
This final step provides a way for the group to reflect on their experiences going through the activity. The group may also draw connections to potential future actions they could take related to the issues represented on their maps. I have found sitting or standing in a circle with the map inside of the circle as the most engaging way to facilitate this step.
The questions below are recommended, but are not the only ones that you could ask.
- What common themes or differences emerged during the process?
- What can we do to learn more about the community? Is there someone with whom we can talk? Is there someplace we can visit?
- Is there any action around shared visions of transformation, or shared experiences of oppression that we would like to explore?
These steps are about adolescents’ ability to make meaning of their community, and treats them as the subjects of their own learning. My experiences facilitating Community Stories have shown me that adolescents grow more comfortable discussing issues that resonate with their individual and collective identities when given the space to do so. While that can take various forms, hopefully, Community Stories will serve as another approach that you can use with adolescents who are looking to change their communities.
The views, information and opinions expressed herein are those of the author; they do not necessarily reflect those of the Council on Accreditation (COA). COA invites guest authors to contribute to the COA blog due to COA’s confidence in their knowledge on the subject matter and their expertise in their chosen field.
Ruben Mina, LMSW
Ruben Mina, LMSW, is a social work community practitioner with close to 15 years of experience in youth development and education. He currently works for the New York City Department of Education alongside an amazing group of folks who are dedicated to achieving equity for students in all schools and districts throughout New York City. His work involves leading workshops for educators on topics like implicit bias awareness, racial equity, and anti-oppression. He also works with educators at the school- and district-levels on creating equitable policies and practices. He serves on the Masters Exam Committee for the Association of Social Work Boards. As a born and bred Brooklyn native, he loves music from any and everywhere, and classic Twilight Zone episodes. He is excited to begin pursuing a doctoral degree this fall.
A big thank you to Shondelle Wills-Bryce, MSW of Sisters Keeping InTouch, inspires, LLC for this guest post!
The peace and serenity of a spring morning is undeniable. Take a moment wherever you are and observe the synergy of nature surrounding you. During my moment, I heard birds chirping, I felt the cool breeze on my arms, and I saw greenery all around. I smiled in amazement, thinking about how nature seemingly effortlessly comes together to bring us beautiful days. I then found myself perplexed about how we as people and we as professionals make “coming together” –aka partnership–so complicated.
Whether you choose to use science, religious beliefs, observation, or a combination of all three, you cannot deny that Mother Nature is the queen of partnership. According to the Oxford dictionary, nature is “the phenomena of the physical world collectively, including plants, animals, the landscape, and other features and products of the earth, as opposed to humans or human creations” (emphasis mine). Each part of nature’s collective does its job without hesitation, and as a result, the system operates successfully.
The system of nature is so effective that even when humans disrupt its natural order, the system automatically adjusts. You may call one such adjustment global warming. However, if Mother Nature could say anything about her adjustment, she might simply say, “I am getting back on track because I am clear about my job and purpose for life on earth.”
In my opinion, the words of Henry Ford describe partnership best:

So, I challenge you to ask yourself, am I clear about my job and my purpose in my partnerships?
Successful partnerships at work
In my various personal and professional roles, I have witnessed the transformational power of partnerships. Some successful partnerships are used for positive impact; others, not so much. Let’s agree to spend our time focusing on the impact and qualities of successful partnerships in order to improve our own.
The annual journal Partnership Matters examines the current thinking and practice in cross-sector partnerships. This journal was developed as a result of the growing recognition that partnerships between business, government, and civic organizations can effectively tackle the social, economic, and environmental challenges of the world. However, based on my experience “aging out” of NYC’s child welfare system, working for the New Jersey Department of Children and Families, and coaching millennial women, I would challenge the journal to include individuals, families, and communities in its examination.
NYC’s Child Welfare System
I was a timid and terrified 15-year-old when the Bureau of Child Welfare (BCW) (today known as New York City’s Administration for Children’s Services (ACS)) placed me in a Bronx group home with 21 other girls. The back story of how and why I was placed in the care of the state isn’t relevant at this time. What is relevant is how the partnerships within the child welfare system helped me become a valuable addition to society.
To wit: The hospital that admitted me did not solely care for my fractured arm.
- The hospital used a collaborative tool to ask me questions about my injury.
- The collaborative tool then triggered the hospital’s need to contact BCW for a closer look at my situation.
- BCW did not solely decide to remove me from the care of my family. BCW spoke to countless community partners (hospital, my school, my family, my neighbors, and me) to make that decision.
The evidence of this successful partnership—and all the communication that it took — was me. Although I was a terrified 15-year-old with limited exposure to the realities of the world, I did not feel lost, and I did not feel alone. After spending six years in the care of BCW, I emerged an educated, responsible, and psychologically sound member of society. That was in large part thanks to this teamwork.
NJ Department of Children and Families (DCF)
15 years after leaving the care of New York City, I began working for New Jersey’s child welfare system (the Department of Children and Families, or DCF) as its Assistant Director of School Linked Services. During my nine years with DCF, my office monitored the distribution and service delivery of $38M in state and federal funds to support school-based prevention and intervention programming. Partnership was key to DCF’s ability to serve children and families effectively, and critical to that was DCF’s strong partnership with the U.S. Department of Health and Human Services, Administration for Children and Families (ACF).
During my last five years with DCF, my office was awarded an additional $6.5M in competitive federal funding. In addition to putting forth and strong comprehensive grant application, I am confident the historical strength and integrity of DCF’s partnership with ACF played a role in the award decision. As a result, the funds expanded services to support NJ’s expectant and parenting youth (including young fathers) with evidence based services. My office had to partner within the department, across state departments, and with the local communities throughout New Jersey:
- Partnerships within DCF included the Division of Children’s Systems of Care, the Office of Adolescent Services, the Division of Child Protection and Permanency, the Division on Women and the Division of Family and Community Partnerships.
- Formal and informal state level partnerships included NJ Department of Human Services (child support and mental health services), the NJ Department of Education, the NJ Department of Labor (employment trainings) and the NJ Department of Health.
- Local partners included community based organizations, local board of educations, universities, hospitals, and representatives of the children, youth, families, and communities targeted for these services.
I will be honest: The time to coordinate, the patience to listen, and the willingness to compromise with these partners was not always easy. However, what made it a little easier was agreed upon goals, clearly documented working agreements (MOUs/contracts), and some good old fashioned open and honest dialog.
As a result of our collaboration, DCF more than doubled its support of expectant and parenting teens from 208 (female students) to 500+ (male and female students). One of the program goals was to prevent subsequent pregnancies while students were in school. I am proud to say that the outcome data reported less than 1% subsequent in-school pregnancies.
Coaching millennial women
At the age of 21, I was no longer allowed to be dependent on NYC’s child welfare system. The system prepared me to be on my own to the best of its ability; however, there was so much I had to learn on my own. I knew if I stayed focused and made all the “right” decisions, I could make it on my own. It worked. I did it–I learned how to survive by getting my college degree and a job to pay for my basic living expenses.
I may have been 28 years old when I felt like I could pause and take a breath. The breath allowed me to no longer worry about failing and worry about what “people” would say. That breath allowed me to truly look at life for its beauty and possibilities. That breath allowed me the luxury of connecting with myself to understand my goals and purpose to thrive in life.
It was about that age that I felt that maybe, just maybe, I was thriving in life. At the same time, I knew then and I know now that there is still so much thriving for me to do. At that age, I didn’t know who in my “real” life to ask for guidance. I’m not sure I even knew to ask. I wonder if my school or the system partnered with me more, I would have known how to really thrive.
What worked for me was finding incredible virtual mentors like Maya Angelou, Oprah Winfrey, Iyanla Vanzant and Suze Orman. The character of each of these women were attractive to me because they were authentic and partnered with the world to make it a better place. Today, I look around and see my former self in young women who have amazing potential but are struggling and doubting themselves.
According Pew Research Center, millennial women (women born between 1981-1996) are better educated and hold a bachelor’s degree at a higher rate their male counterparts. I strongly believe that when the millennial woman takes leadership in her life, she will positively impact her partner, family, and community.
Therefore, approximately two years before I left DCF, I began my own personal development firm, Sisters Keeping In Touch, Inspires (SKIT). In this work, I am committed to partnering with millennial women and those who want to help them not just survive but thrive. This purpose-driven work is accomplished in partnership with millennial women through public speaking, blogging, and facilitated experiences.
In these partnership with millennial women, we work to uplift and strengthen them, so that each can build the personal and professional life of her dreams. When a woman does her building, she will avoid and/or minimize unhealthy relationships with her partner(s), children, finances, friends, and career. We work through an ART process, where she is the artist in her life:

In my work with millennial women, they have felt heard, encouraged, and connected with people and resources needed to thrive. Visit our site to see some stories of success.
These are just three examples from my world of successful partnerships. I am quite sure you have examples of successful partnerships surrounding you as well.
Closing thoughts: Recipes for success
There is an abundance of articles, journals, and opinions about what ingredients go into a successful partnership. My personal favorite is the guidance provided in Don Miguel Ruiz’s book, The Four Agreements:

These four agreements have served me well as a recipe for my success in cultivating and managing partnerships. I challenge you incorporate these agreements in your partnership relationships and experience the transformation. When you do, you may be able to replicate the clear and effective partnership synergy mother nature has shown us in all her splendor.
The views, information and opinions expressed herein are those of the author; they do not necessarily reflect those of the Council on Accreditation (COA). COA invites guest authors to contribute to the COA blog due to COA’s confidence in their knowledge on the subject matter and their expertise in their chosen field.

Shondelle C. Wills-Bryce, MSW
Shondelle C. Wills-Bryce, a master’s level administrative social worker, public speaker and conversation facilitator founded Sisters Keeping In Touch, inspires to help millennial women thrive and not just survive. Shondelle has developed personal resilience having lost her mother to Breast Cancer at 18 months and aging out of New York’s foster care system. Shondelle is the mother of two amazing young women and she is married to her husband and best friend who motivate her each day.
A big thank you to Catholic Charities of Buffalo, New York for this guest post!

We at Catholic Charities Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) Program believe that empathy can create positive change, giving WIC participants the most resources and best experiences possible to live healthier lifestyles with their families and community. Our term for this is called “Participant-Centered Nutrition Services.” With the family and their needs at the center of each interaction at WIC, we can better focus on the nutrition education and resources appropriate to suit them. With this in mind, we created the Shopping Experience Simulation.
The goals of the Shopping Experience Simulation initiative were to:
- Address the barriers encountered by WIC participants during the grocery store experience that prohibit them from using WIC checks to buy nutritious foods;
- Encourage empathy among the staff of nutritionists and nutrition assistants for our WIC families and the issues that they face when using WIC benefits;
- Increase attendance of WIC families at appointments so they may receive nutrition and health information and get referrals to other resources that are available for families in the community ; and
- Identify educational opportunities for WIC staff to improve the WIC shopping experience by providing better nutrition counseling before WIC participants go shopping.
The Shopping Experience Simulation (the Simulation) included three steps: planning, simulation, and debriefing. A team of three staff planned and coordinated all activities in the Simulation. This team met with grocery store management to plan the Simulation, created simulated WIC checks to represent all different kinds of WIC participants, and coordinated which staff would work together. In the Simulation, all WIC participant types were represented: pregnant women, breastfeeding postpartum women with infant, postpartum women formula feeding her infant, and families with toddlers and preschoolers. In the Simulation, staff in teams of two were assigned a WIC participant role, and had 30 minutes to shop with the simulated WIC checks. Immediately after the shopping experience WIC staff attended a debriefing session that included a survey, a group discussion, and a brainstorming session for takeaways.
Planning
In the planning phase, we contacted TOPS Supermarkets as the vendor partner for the Simulation. After phone conversations, we selected the local store and held a meeting with the company executive, store manager, and store management team to review the Simulation plan and establish expectations for all parties. TOPS Supermarket would supply two training checkouts and cashiers to simulate real physical check out of food items, enforcing all WIC policies concerning separating food items, signing and dating checks, and purchasing of approved items. Afterwards, store personnel would replace all simulation food items to proper place in store.
The Simulation was piloted by 13 staff from the Kenmore and North Buffalo WIC locations. Staff would be provided one month of WIC checks. Checks would represent a variety of WIC food packages, including breast feeding mother and baby, infant on specialized formula, participant-requested soy products, and a standard package for child and pregnant woman. Participating staff would have 30 minutes to purchase WIC approved foods as listed on checks, following WIC policies. Staff members were given WIC check folders and food sheets to follow and guide the experience. The staff members were not given the WIC pictorial food guide as an aid. The Store Manager was available for any questions or assistance.
Simulation
Even with all of this structure in place, reality set in. Shelves were bare where baby food should be. Aisles were crowded, and labels were difficult to find to make sure the item was correct. It took over 18 minutes for the pharmacist to unlock the baby formula case. The wait in the cashier’s line was embarrassingly long, as each item had to be checked to make sure it was as written on the check. Staff became frustrated, losing their checks in abandoned shopping carts. If children would have been added to the mix, as they are in reality, it would have been a truer simulation, and almost certainly more frustrating. To ensure an accurate reflection of the shopping experience, the WIC staff immediately completed a written debriefing questionnaire on feelings and experiences associated with the Simulation. Staff then had an opportunity to verbally share experiences and brainstorm ideas for making the shopping experience better, including how to counsel WIC participants to better prepare them for shopping and using WIC benefits.
Debriefing
The debriefing results were tallied and shared with the entire WIC Leadership Team, WIC staff, and the New York State WIC Learning Community. As a result of the Shopping Experience Simulation results, educational action steps were designed to administer this Simulation training to all 107 employees at all 21 sites across the 3 counties that we serve (the Erie, Niagara, and Chautauqua Counties in Western New York). A report with the debriefing data was then e-mailed to executives at TOPS Supermarket to share the impact the Shopping Experience Simulation would have on WIC activities. This partnership and feedback with TOPS Supermarket also generated ideas on how to make the general shopping experience better.
We took challenges in stride, and made adjustments for future Simulations. We noted that too many WIC staff participated at one time, which overwhelmed the small store and training cashiers. To lessen the impact on the store, fewer staff will be trained at one time in the future. Too many checks were given out , and it became too much to handle. In the future, one week of WIC checks will be given to each staff member.
What was learned was more valuable than the resources that went into the execution of the Simulation. This Simulation effectively used resources, as it cost virtually nothing to train the staff. The only cost associated with the Simulation was staff time. Feeling overwhelmed themselves allowed WIC staff to connect with WIC participants. Staff learned to be less judgmental, more supportive, and more open to the needs of WIC families. The WIC Shopping Experience Simulation illustrated how small but effective educational changes can provide better participant-centered nutrition services and make the work of WIC participants, WIC staff, and vendors easier through a more successful shopping experience. Empathy resulting from the experience will give WIC staff an increased capacity to respond to concerns of WIC participants and validate WIC participants’ experience and feelings while shopping with WIC checks.
Embedding lessons learned
As a result of the simulation, several changes have been made to all Catholic Charities WIC office procedures:
- All WIC staff will participate in the Shopping Experience Simulation within the next year and ongoing as more WIC staff are hired;
- All WIC support staff are providing follow-up calls to all new WIC participants, offering support and assistance in any aspect of the WIC process, including successfully using WIC benefits to purchase nutritious WIC foods;
- WIC Nutritionists will spend additional time reviewing the WIC Acceptable Food Cards, including highlighting foods preferred by WIC participants to better prepare them for their selections available when they go to the store;
- All staff will emphasize the importance of WIC check safety and importance of organization and planning in order to have a successful and stress-free shopping experience;
- The WIC Program will collaborate with Vendor Management Agency to act as liaison between the WIC Program and stores to organize simulations. This will help the planning team to accomplish a seamless process for orienting staff on the Shopping Experience Simulation; and
- To make the Simulation more realistic and to develop empathy for WIC participants with transportation issues, the Simulation in the future will include riding the bus or walking a short distance with food purchases.
The Shopping Experience Simulation accomplishes much with little investment. Catholic Charities WIC Program has shared the Shopping Experience Simulation with all other WIC Programs in New York State as an innovative practice. The original team that developed the Shopping Experience Simulation has presented the project on the state level in the WIC Learning Community and for a WIC Conference in Albany, New York. The Shopping Experience Simulation demonstrates a new way of thinking about WIC participants. Walking in their shoes through their experience creates empathy and enriched practices. This has been warmly received in the New York State WIC community. I encourage readers to ask yourself what experiences you can provide your staff to augment their understanding of your clients. Concentrate on your services. Simulating customer service experiences while following our steps of planning, simulation, and debriefing will help your staff gain client perspective. Gathering data from simulation experience will help frame action steps to make your business and services more client-friendly.

The views, information and opinions expressed herein are those of the author; they do not necessarily reflect those of the Council on Accreditation (COA). COA invites guest authors to contribute to the COA blog due to COA’s confidence in their knowledge on the subject matter and their expertise in their chosen field.

Grace McKenzie
Grace McKenzie holds a Master’s Degree in Education from Buffalo State College. For the past fifteen years, she has worked in Community Relations and Outreach for various nonprofit organizations. Currently, she works at Catholic Charities of Buffalo as the Outreach Supervisor for WIC. As a mom, she enjoys family time with her two girls, including exploring nature, tending the garden, visiting museums and family time at home.
Protect your clients, protect your staff, protect your organization, protect your community.
As the virus that causes COVID-19 continues to have a significant impact on our lives, accredited and in-process organizations have asked us how the standards can help them be ready and respond. In this post we will make a few big-picture recommendations about where to start with your preparations, then point out the key standards that might inform your response.
A few quick recommendations
Before we look at specific standards, we have a few recommendations. First, pull your senior staff and members of your governing body together to think about what your organization needs to do be prepared for and respond to the virus. We strongly recommend that you review the CDC’s Interim Guidance for Administrators and Leaders of Community- and Faith-Based Organizations to Plan, Prepare, and Respond to Coronavirus Disease 2019 (COVID-19). This resource is the single best resource we have seen to help you prepare your organization for the inevitable arrival of the coronavirus in your community. The guidance provided is specific and clear and is continually updated as new information emerges.
Second, review and update your emergency preparedness plan and other relevant polices and procedures. COA has several standards that address key preparedness and response issues that accredited organizations will already have in place. These fall under the broad standards categories of human resources management, safety and security, and emergency preparedness. More about these below.
With regard to service delivery: Depending on the types of services you provide and the populations you serve, you are very likely to get multiple communications from federal, state, and county oversight entities, as well as others with specific directives and/or guidance that will directly effect your work at the program level. You will want to merge these varying sources of guidance– some of these will be mandatory–into a form that staff can understand and follow.
It is important also to make this information easily accessible. One organization that serves the homeless mentally ill in upstate New York has been receiving updated virus-related directives from multiple sources almost every other day. Every time one of these is received, the CEO merges the new information into updated procedures and then walks around and replaces the old documents, which have been posted all over the facility, with the newest version. Staff are very busy and aren’t always able to stop what they are doing and check their email to see if new updates have been made to the online procedure manual. So put such critical information right in front of them.
Third, communicate clearly and openly with the people you serve, your staff, and the public. The situation in your locale may be changing quickly. Your clients and staff will be looking to you for guidance. Wild Apricot has a very good blog entry titled How to Create a Crisis Communications Plan for Your Nonprofit that you may find useful.
Communication also includes ensuring that staff know who to go to for answers in rapidly evolving situations. Anticipate that some staff who have decision making authority may become sick. Plan for that eventuality, and make sure that staff know who to go to in their place. This is especially important in larger, multiservice organizations who may provide a variety of different services in multiple locations.
Now lets take a look at some of the key COA standards. Currently accredited organizations will have policies and procedures related to these standards already in place. For these organizations, your task it to review these and update them where necessary.
Review and update your emergency response plan and procedures
Pull out your emergency response plan and procedures (ASE 6.01, ASE 6.02, ASE 6.03) and review them with COVID-19 in mind. If you are like many other organizations, you may not have anticipated a fast-moving pandemic when your plan was developed. Emergency response plans and procedures for multiservice organizations and those providing services at different sites may need to include location-specific guidance for each program site.
Things to consider:
- Clarifying who will communicate with authorities and emergency responders at each program location
- Clarifying and testing your lines of communication to staff, your board, clients, and the public
- Clarifying your responsibilities for persons served with mobility challenges and other special needs
- Do you have sufficient supplies at each site? (I.e. masks, gloves, hand-sanitizer, first aid, first aid manuals, cleaning supplies, disinfectant, toilet paper, food, maintenance supplies, batteries, etc.)
- Is emergency contact information up-to-date for all staff and service recipients?
- Will medications be available for people in residential facilities?
- Are copies of emergency response plans and procedures readily available to staff at all program sites?
- How will programs and administrative offices cope with multiple staff absences due to illness?
- If volunteers perform important functions, how will those functions be done if volunteers are prohibited from entering your program sites?
- How will your programs operate if absenteeism spikes?
Review and update safety and security measures
The standards in ASE 5: Safety and Security address the safety and security of your staff and persons served at your program and administrative sites. Review your most recent safety assessment and any measures that were implemented to address identified issues. Then conduct a new COVID-19 assessment if time permits.
Things to consider:
- Will you need to update or create a visitor policy? (I.e., will visitors be prohibited? Who will be allowed to enter your program sites?)
- Will staff and service recipients be permitted to congregate?
- Will face-to-face staff/client interactions be permitted? If so, under what conditions?
- How quickly can you train staff on updated safety procedures and protocols?
- If you run a residential program, are you capable of quarantining residents? If not, what happens with residents who are ordered to be quarantined? How do you promote/enforce social distancing in congregate care facilities?
Review and update human resource management policies
By the time you read this, many of you will already be under restrictions mandating the closure of all non-essential businesses. Although most of our accredited organizations will be not be subject to those restrictions, most have staff that do not necessarily need to be on-site to perform their jobs. Many of you are scrambling to put human resource policies in place to reflect this new reality. The standard HR 3.02 broadly addresses what may go into an HR policies and procedure manual.
Things to consider:
- Which jobs are critical to the organization’s continued operation? Which can be performed remotely, and which cannot?
- How will critical job functions be performed if key staff are absent due to illness or the need to care for family members?
- Do you have a remote working policy? How will supervision be conducted for remote workers?
- Do your sick time and leave policies reflect guidelines and mandates about virus-related sick time? Does your family-leave time? Do they encourage staff to stay home if they feel sick?
- Is your HR department staying abreast of the latest, rapidly-changing federal and state rules about insurance costs? Are you prepared to help staff understand how new rules apply to them?
Again, the CDC has good, comprehensive, practical guidance for employers: Interim Guidance for Businesses and Employers to Plan and Respond to Coronavirus Disease 2019 (COVID-19).
Review and update technology and information security for remote working
Remote working is as much a technological issue as it is a human resources management issue. The policies and procedures required for RPM 4: Technology and Information Management, and RPM 5: Security of Information should be reviewed and updated if you will be requiring some of your staff to work at home.
Things to consider:
- How will staff securely access work files from off-site?
- How will remote staff communicate with staff who are still working onsite? With each other?
Review and update policies and procedures for technology-based service delivery
The coronavirus has rapidly pushed technology-based service delivery from the periphery to becoming a core intervention modality for many kinds of social and human services. If you are already employing technology-based interventions, take this time to review new rules and guidance coming for the federal government on its use. Then review the standards in PRG 4: Technology-based Service Delivery to ensure that your current practices continue to meet the requirements of the standards.
If you are thinking about employing technology-based interventions for the first time, you need to understand that there are many important factors to consider, including confidentially, security, data collection and transmission, acceptable technologies, licensure, how to work with clients through electronic means, and more. A review of the standards in PRG 4 will give you a frame of reference for what such services look like.
We hope this post helps to bring some of the most important questions into focus for you as you prepare for the coronavirus. The function of accreditation is to build organization’s capacity and resilience through a careful and thorough review of its administration and service-delivery practices. It does this by having you look at what you are doing and how you are doing it, thinking about how you can do things better, and, finally looking ahead so you can be ready for what is coming, both seen and unforeseen.
Be safe.
In light of the ongoing coronavirus crisis, we wanted to highlight some of the resources that we provide on our website, and to provide additional ones, as well. Stay up-to-date on everything happening with COA during the pandemic here.
No matter what role you occupy in the social service delivery continuum, chances are that precautions in the face of COVID-19 have drastically changed the way you work in just a few short weeks. This rapid transition in our lifestyles has led to a deluge of information about how to cope and behave during this time, both personally and professionally. COA has put together a list of references to assist you and your colleagues in navigating all of this news and guidance. We’ve organized the information below by topic:
- General guidance from government agencies
- Guidance for child welfare providers
- Guidance for childcare providers
- Guidance for businesses and employers
- Guidance for healthcare professionals
- Guidance for community organizations
- Guidance on reducing stigma
The Interpretation blog is meant, first and foremost, to be a resource for the COA community. We are continually evolving our blog content to meet the needs of our COA network. If you have a resource, article, or tool that you’d like to see posted, we’d love to hear from you! Reach out to us by email at PublicPolicy@coanet.org.
General guidance from government agencies
It’s important to educate yourself on and follow the guidance of international, national, and local health organizations. The following organizations maintain a collection of resources and information on the spread of COVID-19. COA recommends locating the health agency of your state or territory to find information that is specific to your local community. In addition, make sure that you are signing up for available subscription/distribution lists, where information may be disseminated on an ongoing basis.
- From the World Health Organization (WHO): Coronavirus Disease (COVID-2019) Situation Reports
- From the U.S. Center for Disease Control (CDC): Coronavirus Disease 2019
- From the Canadian Department of Health: Coronavirus Disease (COVID-19): Outbreak Update
- Directory of state and territory health agencies
Guidance for child welfare providers
The US Children’s Bureau shared this letter with the agencies they oversee the in child welfare system. In addition to this letter, the Children’s Bureau is maintaining this webpage with resources related to COVID-19.
Organizations leading the field in child welfare practice and policy have also created resources to assist agencies in navigating service delivery during this time:
- From the National Child Traumatic Stress Network: Parent/Caregiver Guide to Helping Families Cope with the Coronavirus Disease
- From Generations United: COVID-19 Fact Sheet for Grandfamilies and Multigenerational Families
- From Prevent Child Abuse America: Coronavirus Resources & Tips for Parents, Children & Others
- From the National Association of Social Workers: Resources for Social Workers
In addition, The Chronicle of Social Change (now The Imprint) has redirected their reporting to focus on COVID-19 and have posted a number of stories on developments in the child welfare space. We recommend starting with Coronavirus: What Child Welfare Systems Need to Think About.
Guidance for childcare providers
Childcare providers have been deemed essential workers across many regions, even areas with the strictest social distancing regulations in place. This is because we need to ensure childcare is accessible to other essential workers during this time.
Guidance for businesses and employers
There is no doubt that concerns about and restrictions around COVID-19 are impacting how businesses are run. We’ve seen some guidance on how to bear out these changes here:
- From the CDC: Resources for Businesses and Employers
- From the US Department of Labor: COVID-19 Overview
- From the National Council on Nonprofits: The Nonprofit Community Confronts the Coronavirus
Guidance for healthcare professionals
Healthcare facilities are on the front lines of the COVID-19 pandemic. Find resources to help manage resources and protect yourself and your staff below.
- From the CDC: Resources for Clinics and Healthcare Facilities
- From the CDC: Resources for Healthcare Professionals
Guidance for community organizations
Community-based organizations will be integral to ensuring the infrastructure of community needs are able to be met during this time. Fortunately, there are COVID-19 tools available for organizations that serve vulnerable populations:
- From the CDC: Resources for Community- and Faith-Based Leaders
- From the CDC: Resources to Support People Experiencing Homelessness
The National Coalition for Homeless Veterans also has resources specific to each type of services provider they oversee:
- From the National Coalition for Homeless Veterans: COVID-19 Resources
Guidance on reducing stigma
Stigma affects the emotional and mental health of those that the stigma is directed against. Stopping stigma is an important part of making communities and community members resilient during public health emergencies. Even if we are not personally involved with the stigmatized groups, our voice can have an impact.
- From the CDC: Reducing Stigma During a Public Health Crisis
What other helpful resources for managing the COVID-19 outbreak have you seen? Share yours in the comments below.
Thank you to Avi Rudnick, JD, MSW of Chicago House for this guest post!
In the early years of the HIV/AIDS epidemic in the U.S., nearly 100 activists met at the historic Baton Show Lounge to address the dire need for housing for Chicagoans living with AIDS; out of this Chicago House and Social Service Agency was borne as a not-for-profit providing a compassionate response to the disease. Chicago House serves individuals and families who are disenfranchised by HIV/AIDS, LGBTQ marginalization, poverty, homelessness, and/or gender nonconformity. Most of the individuals served have received messages in the past from family and friends that increase shame and stigma regarding behaviors and health status, which can result in a disengagement from services. It was important for Chicago House to choose a service philosophy that helped meet the service recipient where they’re at. Enter harm reduction.
What is harm reduction?

Harm reduction is a client-centered, trauma-informed approach that emphasizes safety and client self-determination. The philosophy dates back to work being done by activists, doctors, programs, and policy-makers in the 1960s and 70s as legal systems all over the globe began to take punitive measures against drugs. An early adopter of the philosophy was the Netherlands who put together commissions assessing whether strict law enforcement was best practice, referring to it as a “balance of harms.” It wasn’t until the 1980s that the collective efforts began to be referred to as harm reduction.
Harm reduction treats the individual as the expert in their own life, service recipients are given the agency to determine whether or how they want to change behavior. While harm reduction does not promote risky behavior, it also does not mandate sobriety as a barometer of success. A concrete example of how this plays out in the real world would be needle exchange programs. Needle exchange programs provide a safe, non-judgmental space for intravenous drug users to exchange their used needles for clean ones. They have been shown to significantly reduce the spread of blood-borne pathogens, such as hepatitis and HIV and, in fact, are associated with increased participation in treatment programs. Instead of focusing energy on the individuals’ sobriety, the programs provide resources to prevent the spread of disease and create a safe space for users. In addition to utilizing harm reduction approaches for addressing substance use, harm reduction is a philosophy that can be applied to many aspects of individual and community life, including, but not limited to: housing, health care, intimate partner violence, and mental health.
Why this philosophy works for Chicago House
Given the individuals served by Chicago House’s marginalized identities, it is not infrequent that one of the earliest and first hurtles is simply earning their trust and building rapport, that is Chicago House’s service providers’ first task. By prioritizing that relationship and putting the individual as the expert in their own life, the service providers help to even out the natural power dynamic that occurs and puts the individual at ease. Together the client and service provider can then explore the individual’s reasons for engaging in high risk behaviors and develop strategies and motivation to engage in safer behaviors (such as engaging in primary care and going on Pre-Exposure Prophylaxis). They inventory the individual’s coping mechanisms and enhance them. Harm reduction supports any positive change, thus putting the individual at ease that they are in a safe space.
Another reason harm reduction makes for a strong service philosophy for the population Chicago House serves is its relationship with trauma-informed care. Most of the clients served by Chicago House and Social Service Agency have experienced some form of trauma in their lives, so it is both fitting and necessary that the agency’s philosophy of care includes a trauma-informed approach to services. Client behavior is considered through the lens of someone who has experienced trauma and is honored as a coping and survival skill, highlighting the clients’ resiliency and ability to adapt which dovetails nicely with harm reduction’s strengths-based approach. Staff members work with clients to establish and maintain a sense of safety and mastery in their environment, something that is often times difficult for individuals with a trauma history, and recognize this as a basic building block for all other interventions.
Implementing harm reduction during service planning
Harm reduction philosophies are infused in the service planning process with clients and work to establish realistic goals regarding housing, health care, income, employment, education, substance use, mental health, etc. Chicago House approaches the creation of service plans with clients as a collaborative process, centering the client as the expert of their own life. While our funders may require that we include certain categories in our service plans, we work with clients on an ongoing basis to develop objectives and strategies to accomplish their goals. For some clients, a goal may be scheduling and attending an appointment with their HIV provider within the next six months, studying for the math portion of the GED exam, or going to the public aid office to apply for the Supplemental Nutrition Assistance Program.
Utilizing a collaborative harm reduction approach allows for changes in life circumstances and for our clients to move through the stages of change without being on the receiving end of shame inducing program requirements that increase fear and the possibility of discharge from programming. If a client does not achieve their goal within the six months outlined in the service plan, case managers use the opportunity to try different interventions, assisting the client in identifying strengths and new possibilities for different goals or a different approach to achieving the existing goal.
Harm reduction-related professional development
Chicago House regularly provides staff with professional development opportunities, such as brown bag lunches. One topic they facilitated recently was Sex Work: Reducing Stigma and Shame. Many of Chicago House’s clients have or are currently engaged in sex work. Instead of asking them to stop or making them feel bad about their choices, providers are being taught about the experience of sex workers so that they are more equipped to support the service recipients.
During this brown bag, staff watched a video of a Ted Talk presented by Juno Mac. She is a sex work activist who fights for sex worker rights and decriminalization of sex work. The discussion was centered on the implications of sex work for specific communities, particularly for trans women of color. Staff reviewed the report, Minority Stress and Sex Work-Understanding Stress and Internalized Stigma by the Sex Workers outreach Program (SWOP) as well as the National Transgender Discrimination Survey, Meaningful Work: Transgender Experiences in the Sex Trade. The brown bag talk wrapped up by reviewing the SWOP guide, Screening 101: Introductory Advice on Why Screening is Important and Some Basic Tips for Avoiding Bad Dates. This screening tool is information that can be directly relayed to the individuals served, providing strategies for reducing harm when engaging in sex work.
Additionally, all new staff members at Chicago House participate in a six-month philosophies of care training series, that includes an in-depth curriculum on harm reduction approaches, with two of the six sessions dedicated to trauma-informed care and motivational interviewing. All program staff members begin this training program within the first three months of employment for a total 12 hours of training on harm reduction approaches.
How other organizations can integrate harm reduction
- Develop and implement ongoing trainings for program staff and administration on harm reduction and related philosophies, such as trauma-informed care and strengths-based approaches.
- Infuse harm reduction language in all policies and procedures, reassessments, service plans, and psychosocial assessments, ensuring to eliminate language that can increase shame and stigma (i.e. not using the terms “clean” and “dirty” when referring to substance use).
- Eliminate the possibility of discharge or ineligibility based upon substance use, sex work, and/or criminal background by focusing on behavior and not stigmatized labels and identities.
The views, information and opinions expressed herein are those of the author; they do not necessarily reflect those of the Council on Accreditation (COA). COA invites guest authors to contribute to the COA blog due to COA’s confidence in their knowledge on the subject matter and their expertise in their chosen field.

Avi Rudnick
Avi Rudnick, JD, MSW began his time at Chicago House and Social Service Agency as a supportive housing case manager in July 2013. Avi stepped into the role of Director of Scattered-Site Housing in February 2016. Avi also facilitates trainings for program staff on harm reduction, trauma informed-care and motivational interviewing. In addition to his role at Chicago House, Avi has been the coordinator of the monthly Name Change Mobilization at the Transformative Justice Law Project of Illinois since 2012. Prior to working at Chicago House and his involvement with TJLP Avi worked as a public defender in Portland, Oregon.
We are all impacted by government spending and regulations beyond our day-to-day work in human services. Regulations empower us as consumers to make informed decisions about our health and safety. They give us peace of mind as employees, that our employer’s practices will be fair and that public spaces will be clean and meet the necessary standards.
We put faith in our political representatives to advance regulation in order to improve the overall welfare of our society. Over time we observe reactive regulation created to address urgent events, gradual regulation to help move the needle on key issues across a country, and preemptive regulation intended to aid the success of future generations.
Let’s explore the role of government regulations and learn more about their value to human services:
Need drives change
First, let’s discuss a historic example of the need for regulation. In September 1982, 12 year-old Mary Kellerman of Elk Grove Village, Illinois, died after consuming a capsule of extra-strength Tylenol. Within a month six more people in the vicinity would be dead and over 100 million dollars’ worth of Tylenol would be recalled from shelves across the United States. These instances amounted to what would be known as the Chicago Tylenol Murders.
The still unidentified perpetrator was purchasing Tylenol in the Chicago area, adding cyanide to the capsules, and returning them to the store. In turn the store was restocking shelves with the returned product and those that purchased and ingested the Tylenol died within an hour of consumption. Johnson & Johnson, maker of Tylenol, distributed warnings to hospitals and distributors and halted Tylenol production and advertising. Police drove through the streets of Chicago using megaphones to warn residents about the use of Tylenol.
In 1983, in response to the incident, Congress passed the Federal Anti-Tampering Bill, also known as the “Tylenol Bill”. The bill made it a federal offense to maliciously cause or attempt to cause injury or death to any person, or injury to any business’ reputation, by adulterating a food, drug, cosmetic, hazardous substance or other product. It also created a FDA requirement that all medications be sold in packaging with tamper-resistant technology.
In the face of a terrifying public safety situation, urgent government regulation was able to ease fears and create a foundation for the way medication is regulated in the U.S. today.
Regulation and our families
An example of regulatory oversight within the human services field is the passage of the Family First Prevention Services Act (FFPSA) by the U.S. Congress in 2018. It marks the largest reform of child welfare financing that has occurred in the past decade. The goal of the child welfare system is to keep all children and youth safe. The regulatory and spending path to deliver that safety has forever been changed because of this legislation.
Today it would be rare to find a human services professional that does not feel the primary initial goal for child placement is reunification with a parent or family member. Acknowledging that to keep kids safe in the long-term we must support families and alleviate issues that may lead to unsafe conditions/removal is widely accepted as best practice. The passage of FFPSA codifies this practice into law and allows funds to be used for family strengthening/preventative practices in child welfare agencies. This is a shift from exclusively funding out-of-home placement, which somewhat incentivized and eased this type of placement.
Though the enactment of FFPSA is a giant leap forward for the field, requiring some states and agencies to change decades of practices and redefining the way we regulate and implement a government program, the overall goal remains the same: to keep all children and youth safe.
Accreditation, a piece of the regulatory puzzle
Accreditation standards serve as a vehicle to implement and verify best practices. COA accreditation is recognized in over 300 instances across the US and Canada as an indicator of quality. In some cases the journey towards accreditation is due to a mandate, which is when states require that certain types of organizations become accredited. Another motivation for seeking accreditation might be due to deemed status, which is when state licensing bodies allow service providers to provide proof of accreditation in lieu of undergoing certain parts of the licensing process. The practice of states/provinces recognizing accrediting bodies is one way that they implement regulation, oversee services, and work to increase quality of services. We recommend checking out the blog post, Help! I’m Mandated! Now What? Choosing an Accreditor to learn more about navigating this topic.
Over time standards are updated to reflect advances in the field, changes in research and practice, quality indicators, and shifts in government regulation. Throughout an organization’s accreditation cycles they are able to evolve with these changes. Accreditation requires that organizations engage their stakeholders, creating an environment for services to adapt alongside the needs of the community. This relationship between accreditors, regulators, and service organizations builds a foundation for continuous quality improvement for both entities, improving outcomes for the clients served.
Conclusion
Instead of approaching government regulations as just another requirement, step back and imagine how they can assist with meeting your organization’s mission. How can these directives support your long-term goals or bolster best practice? As outlined through these examples, regulation is often born out of necessity. These rules can determine a health outcome, the safety of and access to medication, and the path for a child in foster care. At times regulation might seem like another hoop to jump through but in fact it can be a valuable component to your quality assurance toolkit.

In the high-intensity, resource-scarce universe of human services, the service environment itself often gets overlooked, or else overshadowed by compliance concerns. Against the backdrop of serving families at risk, individuals in crisis, and struggling communities, all while trying to keep the doors open, space planning concerns like layout, furnishings, lighting, and décor can seem trivial. Facility design might sound like a luxury, but in reality it has a presence in almost every aspect of service delivery. The evidence is clear. The physical environment can have a profound impact on behavior, mood, perception, and accessibility. When designed intentionally and strategically, your facility can support the work and mission of the organization. Left unexamined, it can limit or even undercut your impact.
Whether you’re opening a new site, considering a relocation, planning a renovation, or just looking for ways to refresh your facility in a way that improves the effectiveness of your services, here are some important issues to consider:
Safe space
The most fundamental concern for every organization is safety. Every facility has to comply with building codes and regulations aimed at protecting occupants from hazardous conditions. Features like emergency exits are specifically designed to promote safety by influencing behavior in the event of a critical incident – such as evacuating during a fire.
Serving vulnerable populations, however, often means preparing for and responding to critical incidents stemming from distress, conflict, and harmful behavior. In recent years suicide prevention has become a focal point for facility planners and is emerging now as a powerful example of how the built environment can be leveraged to save lives. Organizations serving populations at risk for suicide are embracing the imperative to scrutinize all architectural features, fixtures, and materials in the service environment for their potential to become an instrument for harm – specifically as an anchor point or ligature. Shatterproof glass, round-edged doors and tables, breakaway curtain and closet rods, and tamperproof power outlets are just a few examples of features that have been designed to be suicide-resistant. The layout of the service environment can also play a role in reducing opportunities to self-harm; placing staff areas in close proximity to high-risk individuals allows for consistent yet non-intrusive observation.
A trauma-informed approach tells us that identifying and addressing triggers or trauma reminders is key to preventing and de-escalating crisis situations. Organizations must examine both the physical and psychological safety of their facilities and keep in mind that the built environment itself can be a trigger or stressor. An enclosed, restrictive space can often be triggering for individuals with trauma histories or individuals with certain mental disorders, such as schizophrenia; this is often addressed by foregoing corridor layouts and installing glass doors that enable individuals to get a clear view from one service area into the next. Planners also often avoid using the color red to avoid associations with blood, fire, and emergency lights that can trigger a trauma response. Individuals coping with anxiety or PTSD can be overstimulated by patterns, brightly contrasting colors, or other visually complex designs; neutral or softer colors with more subtle transitions are therefore generally more appropriate for therapeutic environments.
While safety is imperative, there are plenty of other ways the built environment intersects with organizational goals and priorities. Now that we’ve looked at how the physical environment can reduce suicide, harmful behaviors, stress, and aggression, we can turn to how it can reinforce and encourage positive behavior and promote better client outcomes.
The client experience
A well-planned facility should complement your organization’s work by ensuring that individuals and families feel safe, supported, and in control while they are receiving services. To learn more about how organizations use the built environment to support their work, we spoke with Children’s Institute, Inc. (CII) in Los Angeles, a COA-accredited organization that provides a broad array of mental health, early care and education, child welfare, family support, and youth development services to children and families – who are also currently in the process of relocating one of their sites and constructing a new campus.
A client-centered approach informs many of the crucial decisions CII has made in identifying and designing their new facilities. “We thought about how it would affect the client’s experience, being on one floors or two,” says COO/CFO Eugene Straub. CII has been careful to ensure that their facilities are welcoming to both clients and staff. “The goal is building a sense of trust and security. The last thing you want to do is make anyone feel uneasy.” Improvements have also been made to existing sites where the space was not meeting families’ needs. “We had a nice lobby and waiting areas but there were no activities, and we looked for ways to change that and make the space more inviting and inspiring.” Now CII’s once-empty waiting areas include a lending library and creative space for children and families to use.
What are some ways that your organization could find inspiration and ideas when planning facilities? Your service recipients, staff and community are a great resource for ideas and a great place to start. Organizations should always look to their service recipients and their communities for ways to enhance their service environment, and tailor their facilities to the unique needs of the service population and to their service model. For example, a residential facility for individuals with schizophrenia can provide some relief to residents coping with paranoia by orienting beds and desks to face the door. A youth development program for children with autism spectrum disorder, who often struggle with spatial navigation and wayfinding, should consider applying visual cues to transitional spaces. Every organization’s approach to designing an effective and supportive service environment will be unique and depend on their scope, service population, service model, and culture. But there are a few universal design features that facility designers and environmental psychologists agree contribute to a calming, welcoming, and therapeutic service environment:
Nature equals nurture
Studies have consistently shown that access to nature, whether physical or visual, has a calming effect. Treatment facilities often situate themselves in a natural setting for this reason, but any organization can look to existing assets to bring to their full potential, such as a small outdoor space that can be converted into a courtyard or garden, or installing windows to take advantage of a good view. Organizations that are truly limited can still make enhancements by incorporating plant life into the decor and displaying nature and landscape art, which have also been demonstrated to have a positive and calming effect on mood.
Let the sun shine
Sunlight triggers the release of serotonin, which boosts mood and focus. Research also indicates that the ability to identify time of day through observed sunlight is conducive to re-establishing perception and natural thinking while minimizing disorientation. Natural light also makes small spaces appear larger and more open than they are. Organizations should ensure that they’re maximizing and not obstructing their natural light, such as by moving furniture away from the windows, using window coverings that filter rather than block out sunlight, and opening up any doors and windows that would allow natural light to pass through the facility. Transom lights (windows built into the space above a door) and skylights are also examples of architectural features that maximize sunlight while still preserving privacy.
Power to the people
A client-centered and trauma-informed approach to services stresses the importance of giving service recipients opportunities to have a voice in their service plan and at each stage of service delivery. For survivors and individuals coping with past trauma, opportunities to take control and make their own choices are important exercises in self-empowerment and essential steps on the road to recovery. Current best practice regarding residential facilities stipulates that residents should already be encouraged to personalize and decorate their own space. However, when possible, personal choice should also be extended to the environment by giving service recipients the power to customize lighting, temperature, acoustics, or furniture arrangements. To balance flexibility with safety, facility planners often choose furniture that is too heavy to be thrown or used as a weapon, but that can still be moved around and reconfigured, which gives individuals (or groups, in communal settings) autonomy to situate themselves where they feel safest.
No place like home
Experts typically agree that a safe, therapeutic, non-institutional and homelike environment is the best setting for residential treatment. Some strategies that designers employ to make a facility more warm and inviting include using upholstered rather than hard furnishings to invoke a softer, cozier feel, and mixing and matching a cohesive array of furnishings to avoid a uniform, institutional look. Given that “home” is a cultural construct, cultural competency is vital to ensuring that your environment meets the definition of “homelike” for your service population.
Of course, “home” is about more than just furniture — it’s also about people. When designing or evaluating a facility, organizations must consider not only the service recipient, but their support network. Because an engaged and committed support network is one of the most important contributing factors to positive client outcomes, service environments need to promote and facilitate their ongoing involvement. Organizations should be mindful that an imposing service environment can discourage or inhibit the service recipient’s support network, and evaluate whether their facility accommodates and encourages visiting family and friends as well as any collaborating service providers. Is it intimidating for visitors to access or navigate the facility? Are there welcoming spaces for residents to spend time with their visitors, or to have private conversations?
Supporting your staff
Getting your space to work for your service recipients also means ensuring that it works for your workers. As with service recipients, the environment influences workers’ behavior, mood, and functioning – which in turn impact performance and productivity, and your organization’s effectiveness. In human services, an ineffective environment undermines not only your bottom line but your mission.
The human services field also faces significant workforce challenges – namely recruitment, retention, and secondary trauma. Qualified workers are in short supply, in no small part due to poor funding and stigmatization of the service population. Staff shortages and the difficult nature of the work, which often manifests as secondary or vicarious trauma, lead to burnout and to high rates of turnover. Finally, worker turnover negatively affects client outcomes.
These workforce challenges have been at the center of the design and planning process for Children’s Institute, Inc.’s new offices. With the aim of promoting collaboration and “addressing the adverse effects of the work itself”, CII decided to eliminate cubicles in favor of a communal, team-driven open plan layout that will allow staff to support one another, celebrate their successes together, and foster staff resiliency. Straub observed that the cubicle layout often forces staff “to go from meeting with clients to sitting at their desk by themselves” and process their experiences in isolation. The intent of the new layout is to encourage workers to “have more of a shared experience and focus on wellness and self-care both individually and with each other”. The new offices also feature “decompression zones” – calming work-free spaces for staff to recover, including through meditation and yoga, as well as larger common areas, kitchens, and breakrooms. Evolving workplace norms mean that “the younger workforce wants an office space that fosters support and feels less corporate and more collaborative,” Straub explains, making these amenities not just “perks”, but rather, vital resources that will promote staff wellness and strengthen recruitment of valuable staff.
CII is also allocating space for “drop-in” staff – workers from other sites who are out in the field will be able to use nearby CII offices as a landing spot in between client visits. Straub envisions that this increased “cohabitation” will stimulate knowledge and resource-sharing and enhance linkages for families and continue to build the culture of the agency. Emphasizing the importance of “collaborating with the end user,” CII has also been careful to engage staff in the facility planning process, bringing all staff to tour the new space before signing the lease and soliciting feedback about the environment as part of annual employee surveys. Continuous assessment of a new or revamped workspace is not just good quality improvement practice, it also ensures that the organization identifies and addresses any unforeseen effect on employee functioning. For example, in an evaluation study of behavioral health facilities, researchers discovered that staff in a new facility that had been designed to promote client-staff engagement were experiencing greater burnout in response to the increase in client interactions.
Strategic plans to building plans
Creating a safe, effective, and supportive service environment requires the organization to approach the physical environment as part of its mission. It calls for not only commitment and investment, but also a shift in attitude — away from “being happy just to get the space”, as Straub says, and towards leveraging the space to influence how the organization’s operations are experienced and perceived. By tying together their facilities, mission, and strategic plan, CII’s ambitious expansion project received enthusiastic support from its board and funders. Straub sees the new campus as “an opportunity to create organic change” by leveraging the space to build partnerships with the community; plans are already underway to co-locate with other providers and host community taskforces and other grassroots organizing initiatives.
As much as we’d like the primary takeaway here to be “good facility design is not about aesthetics”, it bears noting that a well-designed facility achieves through its appearance two invaluable objectives: firstly, it destigmatizes the organization’s services and service recipients, and secondly, illustrates the depth of the organization’s commitment to the community.
Tell us in the comments: How has your organization used its facilities to support service recipients and staff? What would you change about your current service environment?
Further reading
Building Better Behavioral Health Care Facilities
Rethinking Behavioral Health Center Design
Designing for Post-Traumatic Understanding
6 Behavioral Health Design Trends
Can a Frank Gehry design help change the dynamic of Watts?
You are probably familiar with the ripple effect. The term refers to a sequence of events that is triggered by a particular incident or occurrence. The most common example is dropping an object into a body of water…let’s say a stone in a lake. Once it falls, the stone causes a series of waves that spreads across the body of water, the waves ever expanding their reach. The metaphor is often used to describe the potential impact that our actions have on others and the world around us. At times, we may not even be aware of the ripples that we set in motion.
There is no better way to describe the current opioid epidemic. Opioid dependence doesn’t just affect the individual user; it touches the lives of those around them, leaving its mark on children, family members, and friends. And it doesn’t end there. The ripples grow and extend to countless sectors.
One system that is feeling the impact of the opioid epidemic is child welfare. Reports from public officials, advocates, and those working in the field echo the same sentiment – the current crisis is overwhelming. As opioid abuse continues to increase nationwide, the demand for foster care placements is also on the rise. This leads us to wonder what is the relationship, and what does it mean for families and future generations of children?
In recognition of National Foster Care Month, this article will shed light on the connection between the opioid epidemic and child welfare and contribute to the ongoing dialogue on how policy and practice can better support those working with families entrenched in this devastating crisis.
The scope of the problem
Opioid use disorders and fatalities continue to rise
There has been a sharp uptick in the use of opioids since 2010. According to SAMHSA, in 2016, 2.1 million Americans had an opioid use disorder (OUD). As that number continues to rise, so does the number of fatalities. The Centers for Disease Control and Prevention (CDC) reports that 115 Americans die from an opioid overdose every day.
The number of children who have parents struggling with OUDs is unknown. However, a 2017 analysis yielded that 1 in 8 children resided with at least one parent who had a past year substance use disorder (SUD). The report also found that 1 in 35 children lived in a household with at least one parent who had an illicit drug use disorder. Unfortunately, it leads us to consider that parents are among those that we lose to the opioid crisis on a daily basis.
Foster care placements are increasing
Concurrently, as reports of opioid use rise, the demand for foster care placements across the country has also grown. The number of children entering foster care was on a steady decline for more than a decade; however, the tide shifted in 2012. From fiscal years (FY) 2012-16, the number of children in foster care nationally grew by 10%. While individual states varied, more than two-thirds experienced a surge in foster care caseloads during this period. Six states – Alaska, Georgia, Minnesota, Indiana, Montana and New Hampshire – saw foster care populations rise by more than 50%.
More children are residing with grandparents and relative caregivers
Another recent development is the growing number of grandparents taking on the primary caregiver role. Generations United reports that about 2.6 million children – 3.5% of all children nationwide – are being raised by grandparents or relatives across the country. When we look at the data, 32% of children in foster care are being raised by kin, more than previous years. And that may be just the tip of the iceberg. It is estimated that for every child in foster care with relative caregivers, there are 20 children being cared for by grandparents or other family members outside of the foster care system.
Parental substance abuse is a contributing factor for out-of-home placements
What contributes to the need for out-of-home placements? According to the latest national data, parental drug abuse is a factor in roughly one-third of all child removals. While the proportion of children entering foster care due to these circumstances appears to have remained steady over the past few years, it is increasing. Looking across the different categories for removal, drug abuse by a parent had the biggest percentage point growth between FY 2015 (32%) and FY 2016 (34%), which is notable in the face of the current epidemic.
Connecting the dots
So…is there a relationship between the opioid epidemic and child welfare, and if so, what is it? It’s complicated.
Given the timing of these trends, it is hard to imagine that increased opioid use doesn’t play some role in rising foster care caseloads. A recent national study found that counties with higher substance use indicators (drug overdose deaths and drug-related hospitalizations) have higher rates of foster care entry, indicating a relationship between child welfare caseloads and substance use prevalence. However, we have to remember that correlation does not automatically equal causation (proof that what you learn in statistics will come back around) since we can’t control for all demographic and socioeconomic factors and their potential influence on out-of-home placements.
Even though the increase in foster care and relative care placements has been attributed to the opioid epidemic, empirical evidence to prove cause and effect is lacking. This is in part due to the way that the federal government and states track data on child removals, more specifically the contributing factors. For example, there is national-level data on the number of children being removed due in part to parental drug abuse, but it isn’t broken down in a way that shows what type of drug was being abused. Therefore, there is no way to know how many foster care placements stemmed from opioid abuse versus the abuse of another type of illicit drug.
Nonetheless, public officials, advocates and others working in the field are making a direct link between the opioid crisis and increased demand for out-of-home placements. Anecdotally, there are similar accounts across states of the opioid epidemic and its impact on communities. Child welfare agencies are seeing more children come into care because of parental opioid abuse, and children entering the foster care system are getting younger and younger. It has been reported that there aren’t enough foster homes to meet the growing need. Caseworkers are feeling overwhelmed by growing, multifaceted caseloads.
What does this all mean for children and families?
Substance use disorders impact on families
Let’s take a step back. To understand the ripple effect of the opioid epidemic, we have to first look at how parental substance abuse impacts child and family outcomes. At a foundational level, parents struggling with a SUD may not be able to provide for a child’s basic needs (e.g., appropriate supervision or nutrition). Equally troubling, a child can be deprived of emotional support and positive attachment, critical factors in healthy childhood development. Inconsistent parenting inevitability hinders stability in the home. For a child, life can become chaotic and unpredictable, both of which are associated with negative outcomes. That is why parental substance abuse is a known risk factor for child welfare involvement. A 2016 study found that when compared with their peers, children whose parents faced SUD-related issues were three times more likely to experience abuse (physically, sexually, or emotionally) and four times more likely to experience neglect.

Parental substance abuse and child trauma
We know that trauma experienced early in life can adversely impact a child’s development and have long-term health consequences, and parental substance abuse is a one form of childhood trauma (aka an adverse childhood experience or ACE). Often, substance abuse is compounded with other types of adversity, making the severity of potential negative outcomes even worse.
Research shows that history has a way of repeating itself. Children who grow up with complex trauma are more likely to struggle with substance-related issues. One study found that individuals with five or more ACEs were seven to ten times more likely to have issues with illicit drug use. Other explorations into the topic have yielded similar results. There are a host of reasons why people with past trauma experience are more vulnerable to developing a dependence on substance use. While not all children will experience such consequences, the risks to future generations are far too great and warrant immediate intervention. In order to break the cycle, we have to find a way to address the opioid epidemic that is trauma-responsive.
The role of child welfare
The child welfare system is poised to be a catalyst for change. Agencies are tasked with protecting children from maltreatment, abuse, and neglect, and in-home services play a critical role. In-home services are aimed at promoting the well-being of children by ensuring safety, achieving permanency, and strengthening families. When faced with familial challenges, keeping children with their parents is optimal (as long as it is safe and appropriate). Children do best in families with the support of at least one caring adult. Even in crisis, children can thrive when the right protective factors are in place. Removing a child from his or her home disrupts daily life and expectations. All of that instability can be traumatic. The stress that stems from coping with parental loss can have long-lasting effects on a child’s emotional, behavioral, and academic outcomes.
Parental substance abuse has long been an issue for child welfare agencies, one that is now amplified by the recent opioid epidemic. Child welfare agencies across the country are inundated with high caseloads. The complexity of the cases given the unique circumstances and service needs of families battling opioid dependence are adding another layer to an already challenging situation. Not to mention, family stabilization and/or reunification is complicated (contender for understatement of the year). Despite what we know about keeping families together, having children remain with their parents may not be in their best interest due to the impact that substance abuse can have on parenting, making out-of-home placements the safest option. What’s more, reuniting children with their parents can be tricky given ebbs and flows of recovery. The tug-of-war that this creates for caseworkers can be challenging to navigate. So, how do we support those working with families experiencing the crisis firsthand?
Where do we go from here?
Implement what works for families
States and localities are getting creative and implementing interventions that have proven effective for families, recognizing the trauma associated with parental substance abuse. There is ample support for family-centered treatment for substance abuse, including opioid dependence. Additionally, program models that focus on systematic change and cross-system collaboration have also been linked with favorable outcomes.
- Sobriety Treatment and Recovery Teams (START) is an intensive, integrated program for families experiencing co-occurring substance use and child maltreatment. START launched in Cleveland, Ohio in 1997 and extended to Kentucky roughly a decade later. The program matches up specially trained child protective services workers with family mentors (peer support specialists in recovery), behavioral health treatment providers, and the courts. The goals of the program are to ensure child safety and reduce the need for out-of-home care. A 2012 study on the impact of START on family outcomes found that mothers who participated achieved sobriety at a higher rate than those in more traditional treatment programs. Children were also placed in the custody of the state at half the anticipated rate.
- Medication-assisted Treatment (MAT) – an approach that combines medication with counseling and behavioral therapies – is a best practice, and has been linked to decreases in negative outcomes (e.g., opioid use, opioid-related overdose deaths, criminal activity, and infectious disease transmission) and increases in social functioning and retention in treatment, two factors that play heavily into improved parenting skills. MAT has also been found to be effective in providing care for pregnant women who struggle with opioid dependence. Despite some misconceptions in field out the approach, MAT has been associated with improved prenatal care, reduced illicit drug use, and better neonatal outcomes.
- Family Treatment Drug Courts (FTDCs) are specialized courts that respond to cases of abuse and neglect involving caregiver substance misuse. Using a family-friendly approach, FTDCs combine judicial oversight and comprehensive services by bridging together substance use treatment, child welfare services, community supports, and the court system. The unique model balances the rights of both children and parents and aims to create safe family environments while treating the parents’ underlying substance use disorder. In 2015, there were a reported 300 FTDCs across the country, with models and implementation varying state-to-state. The benefits associated with FTDCs include higher participation rates and longer stays in treatment (when compared with non-FTDC participants). The model also yields positive child outcomes; children reportable spend less time in out of home care and are more likely to be reunified with their parent(s).
Support for child welfare agencies and caseworkers
Child welfare agencies are first responders to families in crisis. Caseworkers can encounter stressful or traumatic experiences working with families opioid dependence, witnessing the aftermath of a parental opioid overdose is just one devastating example. That is why supporting frontline staff is imperative.
Provide Specialized Training
Reports indicate that there can be gaps in knowledge among caseworkers around the needs of families with substance use issues and the treatment of opioid use disorders. Training and support in these areas is critical for those working in the field. Additionally, specialized training around recognizing and responding to trauma and trauma-informed care practices is needed when working with families impacted by opioid abuse, as there can be long-lasting negative effects for children if trauma symptoms go undetected and untreated.
Promote Workforce Well-Being
Organizations should employ strategies to reduce secondary trauma and burnout in order to promote workforce well-being. Approaches to reducing the adverse effects of include:
- helping staff identify and manage the difficulties associated with their respective positions;
- encouraging self-care and well-being through policies and communications with personnel;
- offering positive coping skills and stress management training; and
- providing adequate supervision and staff coverage.
Encourage Systems Coordination
Families with substance use issues frequently face other risk factors. Collaboration with other service providers is crucial in helping link parents and their children to the services that they need. The surge in opioid use has trickled into a number of child and family-serving systems. As such, agencies should take steps whenever possible to develop partnerships in their communities to support the work.
Allocate Federal Resources
The crisis is too far-reaching to not have a comprehensive, coordinated federal plan of action in place. Despite declaring a public health emergency, we have yet to devote the level of funds that are needed address opioid dependence. While social service providers and child welfare agencies continue to try and mitigate the impact on a local or state level, the importance of allocating appropriate federal resources to support these efforts cannot be overlooked.
For example, the Maternal, Infant and Early Childhood Home Visiting Program (MIECHV) funds home visiting programs that aim to promote positive parenting practices and healthy parent-child interactions. These programs can also link parents struggling with substance dependence to appropriate treatment providers. Research shows that no matter what level of care is needed, the most beneficial approach is the one that treats families together. MIECHV could help address the unique service needs of the growing number families impacted by opioid dependence.
The Family First Prevention Services Act (FFPSA) may also be a way for federal resources to help child welfare agencies respond to the epidemic. FFPSA is poised to dramatically overhaul the child welfare system, putting federal dollars toward prevention programs and interventions aimed at keeping families together. Substance use treatment programs are among the services that can be prioritized through the restructuring of funds. Additionally, given the increased demand for foster care and relative caregiver placements, advocates are calling to strengthen foster parent recruitment and retention efforts and kinship navigator programs. Increasing capacity in these areas will in turn aid child welfare agencies in finding safe, appropriate placements for children impacted by the current crisis.
There are a variety of other ways that programs and policies could provide relief at a national level; however, equally important is the need for improving data collection across various systems to make informed and evidence-based decisions.
The thing about the ripple effect…
It is hard to stop once it gets put in motion. But that doesn’t mean we shouldn’t try. While the current crisis is overwhelming, there are proposed solutions, ones that can positively impact families and change the course for future generations.
We encourage you to share your thoughts on this important issue. How has the opioid epidemic impacted your community and the children and families you serve? What has been the response? Share your feedback in the comments below!
Dr. Robert Block, former president of the American Academy of Pediatrics, has been widely quoted as saying, “Adverse childhood experiences are the single greatest unaddressed public health threat facing our nation today.” That is a statement that many would agree holds true at this very moment, and one that cannot be ignored.
April is child abuse prevention month, and there is no better time to raise awareness around the long-lasting effects of child abuse, neglect, and other types of childhood trauma. This article will explain Adverse Childhood Experiences, share relevant findings from the CDC-Kaiser Permanente Adverse Childhood Experiences (ACE) Study, and explore how to put science into practice in order to mitigate the impact of early adversity and toxic stress.
What are Adverse Childhood Experiences?
Adverse Childhood Experiences or ACES are traumatic early life events that can lead to negative health outcomes as adults. Much of what we know about ACEs stems from the CDC-Kaiser Permanente Adverse Childhood Experiences (ACE) Study, conducted between 1995 and 1997, which examined 10 types of childhood trauma and their impact on long-term health and well-being. Researchers identified three categories of childhood trauma: abuse, neglect, and household dysfunction. The findings were shocking.
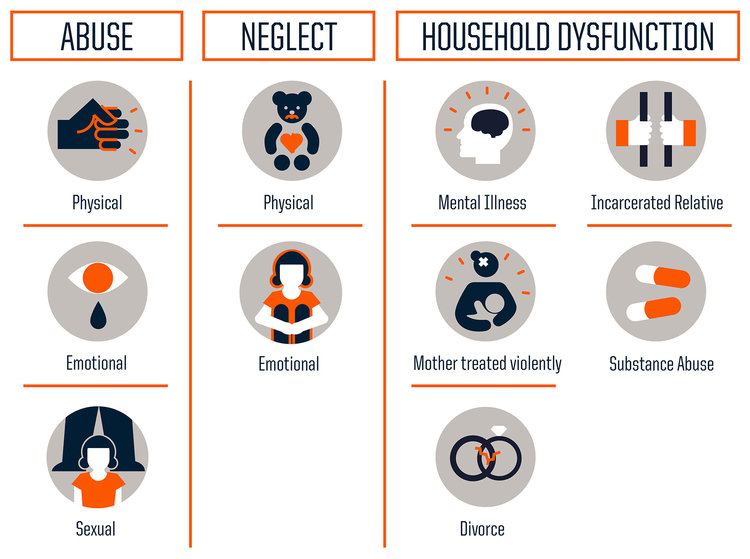
The study concluded that the more adversity one experiences earlier in life, the greater the risk of significant physical, emotional, and social consequences in the future. Now, you may be thinking – Why is that so shocking? A difficult upbringing being linked to hardships down the road, what is groundbreaking about that? Well, it is the prevalence at which ACEs occur, and in turn the impact that has on the population. Studies are often criticized for their self-selecting biases, however this investigation challenges that concern. The 17,000+ study participants were predominantly white, middle- and upper-middle class; most were college-educated and had stable jobs and heath care. They represent a group that we don’t typically associate with adversity, showing that trauma has no boundaries and is more common than we think.
Let’s break it down…
Everyone has an ACE score of 0 to 10, with each type of trauma counting as one regardless of the number of times it occurs.
According to the study, nearly two-thirds (64%) of adults have experienced at least one type of childhood adversity. ACEs increase the risk of: chronic disease and health issues, mental illness, engaging in risky behaviors (smoking, substance misuse, and unsafe sexual activity, for example), inadequate social skills, poor academic achievement and/or work performance, and intimate partner violence. The study also showed that ACEs cluster, meaning that if you have one there is a good chance (87%) that you have another. Almost 40% of participants reported two or more ACEs and roughly 12.5% experience 4 or more ACES. The higher your ACE score, the worse the outcomes.
When you look at each type of trauma and look at the prevalence of specific ACEs, the most dominant ACE experienced by participants was physical abuse (28%), followed closely by having a family member with a substance use disorder (27%). However, it is important to note the type of trauma does not impact the outcome per say. To the brain stress is stress; therefore, it doesn’t matter what type of adversity you face, the health consequences will be the same.
When a child experiences trauma, their cognitive functioning and ability to cope with tricky and icky (technical terms) emotions are compromised. Repeated exposure to traumatic events in childhood or prolonged adversity without appropriate adult/caregiver supports negatively affects the way the brain develops and functions; this is known as toxic stress. Toxic stress can be harmful on one’s physical and mental health, yielding undesirable outcomes later in adolescence and adulthood.
Why does this occur? Stressful or traumatic events early in life have a direct impact on a child’s brain development. The brain experiences rapid changes during the first five years, especially from birth to age three. During this informative time, the brain and its neural pathways are susceptible to external factors. While occasional stress is part of a child’s healthy development, chronic stress can negatively affect learning, growth, and behavior. This is in large part due to the overload of stress chemicals and their influence on the brain. When we feel threatened, the body activates our stress response systems and releases stress hormones (e.g., adrenaline and cortisol). Stress reactions and chemicals are meant to protect us, but too much can have the opposite effect. Enter toxic stress. Extended activation of stress response systems in early childhood can disrupt the structure of the brain and the way it communicates with the body, which can lead to major health issues in the future.
Building resilience
The brain is constantly changing in response to the environment; it is kind of like a chameleon in that way. This adaption is key to facilitating positive change in the face of toxic stress. Creating safe, stable, nurturing relationships and environments are critical to mitigate and prevent the consequences of childhood adversity. While ACEs have the potential to be long-lasting, they don’t have to be; we have the tools to help children thrive in the face of adversity and go on to meet their full potential.
A strong (and continuously growing) literature base has demonstrated that building resilience can help negate stress-induced changes in the brain. Resilience is the “process of adapting well in the face of adversity, trauma, tragedy, threats or significant sources of stress”. Experts in the field of child trauma convey that one of the biggest determinants in being resilient is having nurturing and supportive relationships with adults in one’s family and community. Dr. Bruce D. Perry, a childhood trauma guru, considers “the more healthy relationships a child has, the more likely he will be to recover from trauma and thrive.” And it’s true, adult-child relationships play a significant role in helping children cope with challenges. If stress reactions are time-limited and buffered by protective adult relationships, a child is able to recover and learns how to adapt in difficult situations. That is why high-quality, evidence-based parent education, home visiting programs, and parenting practices are so important. These interventions emphasize the power of familial relationships, caregiver bonding, and positive social interactions. Just as critical are protective factors and their role in strengthening families and preventing trauma. Studies have shown, and continue to investigate, the ways in which different protective factors promote optimal child development. And while intervention can occur at any time – there is no magical cut-off age – there is clear evidence that shows the earlier the better.
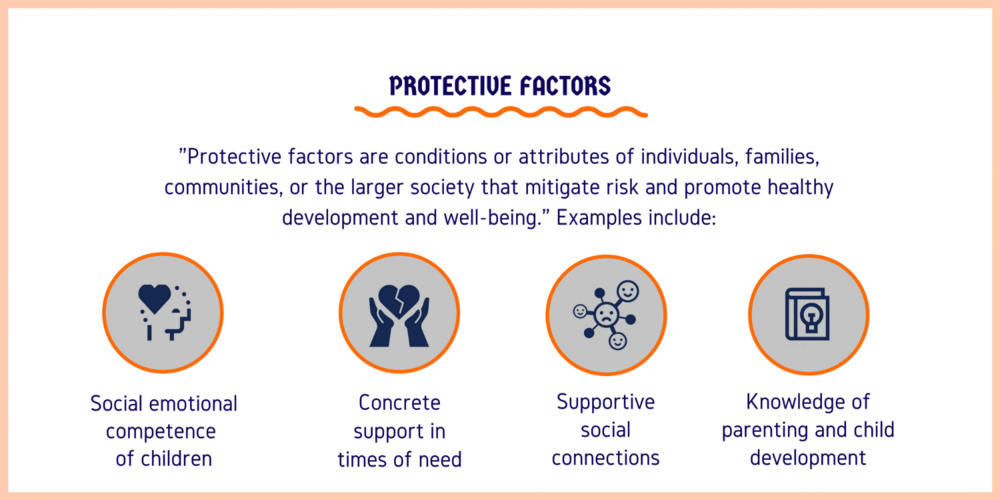
There is hope
It’s true that the findings from the ACE Study don’t leave you feeling warm and fuzzy. In fact, at this point, you may be wondering if there is any hope or if we are all doomed. Fear not! This is actually the exciting part (hear me out…).
The ACE Study findings are paving the way for innovative solutions to a public health crisis. It’s cutting across sectors and systems to bridge services and advocacy, and encouraging individuals and groups to collaborate and communicate like never before. From pediatricians to social workers, people in communities nationwide (and internationally) are using ACEs science to join forces and better the lives of children and families. Here are just a few examples:
- The Center for Youth Wellness developed an ACEs screening questionnaire and protocol for pediatric care providers to target more effective early intervention strategies.
- In Manchester, NH, a joint-response team a – Adverse Childhood Experiences Response Team (ACERT) – is bringing together law enforcement, mental health professionals, and community providers to respond to the service needs of children who have been exposed to violence.
- Lincoln High School in Walla Walla, WA incorporates ACEs into their work with students, more specifically their approach to school discipline.
- Trauma-free NYC, a university-community partnership, aims to raise awareness of ACEs and design and promote training and learning opportunities for the larger NYC community.
- Community members and practitioners in Raleigh, NC came together to watch a film about the science of ACEs, Resilience, and have an in-depth discussion around how systems can better address children who have experienced trauma.
A call to action
In her 2014 TED talk on childhood trauma, Dr. Nadine Burke Harris closed in saying, “The single most important thing that we need today is the courage to look this problem in the face and say, this is real and this is all of us. I believe that we are the movement.” Indeed we are. We are the change makers that can combat the effects of childhood adversity. Knowing what we now know, how do we move forward?
Continue to raise awareness
We must continue to raise awareness, not just of the long-term outcomes assocaited with childhood trauma, but also the power of early intervention. Recently, 60 Minutes did a piece on the impact of childhood trauma, highlighting the impactful work of organizations like SaintA and Nia Imani Family, Inc.. The eye-opening conversation was facilitated by Oprah Winfrey…yep, Oprah. The importance of stories like these in mainstream media cannot be understated. We know that when Oprah talks, people listen. Look at the traction that this one segment has gotten over the past month. It’s been invigorating.
Want another example? Sesame Street collaborated with the Robert Wood Johnson Foundation to launch an initiative to help children manage traumatic life experiences. Who better to take on the task than the beloved Sesame Street Muppets? The characters are loved by children and adults alike. An array of research-driven materials have been created through the partnership and are available to children, parents, and professionals. The content is truly original and inspired – it even includes Muppets modeling coping strategies – and emphasizes the power of resilience in the face of adversity.
Now, recognizing that we all don’t have access to Oprah, Big Bird, or a national TV network (wouldn’t that be awesome though?), it is important to take to the platforms we do have at our disposal to spread our message. Post an article on your organization’s Facebook page, email your colleagues, tweet at your community partners…Connecting with diverse audiences ignites new and ongoing conversations around where we are, what we know, and what we can do.
Become trauma-informed
Trauma-informed care is no longer the exception, but instead the expectation. It’s about reframing the conversation from “What’s wrong with you?” to “What happened to you?” There are a great deal of resources out there that provide excellent guidance on becoming trauma-informed, both in clinical practice and at the organizational level. Here are a few that you may want to check out:
- ChildTrauma Academy
- Child Welfare Information Gateway – Trauma-Informed Practice
- National Child Traumatic Stress Network (NCTSN)
- National Center for Trauma-Informed Care and Alternatives to Seclusion and Restraint (NCTIC)
Promote shared learning
Many in the field have been advocating for the implementation of programs and policies that address ACEs, calling for more data and additional research to better target prevention efforts and supports. The fact is that while the ACEs may be new to some, others have been implementing innovative trauma-informed, resilience-building practices in their everyday work to create positive change. We have presented a few examples, but there are many more being spearheaded by individuals, organizations, systems, and communities nationwide. Shared learning is crucial to creating and maintaining a movement.
Be part of the movement
And with that…we want to hear from you. What do you think about the ACE Study and the findings? How are you addressing the needs of children and families who have experienced trauma? Are you implementing innovative trauma-informed practices at your organization?
Share your thoughts in the comments below!